Beijk Marcel A M, Palacios-Rubio Julián, Grundeken Maik J D, Kalkman Debbie N, De Winter Robbert J
Department of Cardiology, Amsterdam University Medical Center, University of Amsterdam, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands.
Cardiology Department, Hospital Universitario Son Espases, Health Research Institute of the Balearic Islands (IdISBa), 07120 Palma, Spain.
J Clin Med. 2023 Feb 7;12(4):1311. doi: 10.3390/jcm12041311.
Acute myocardial infarction (AMI) with occlusion of an unprotected left main coronary artery (ULMCA) is a rare condition with a high mortality. The literature on clinical outcomes after percutaneous coronary intervention (PCI) for cardiogenic shock secondary to ULMCA-related AMI is scarce.
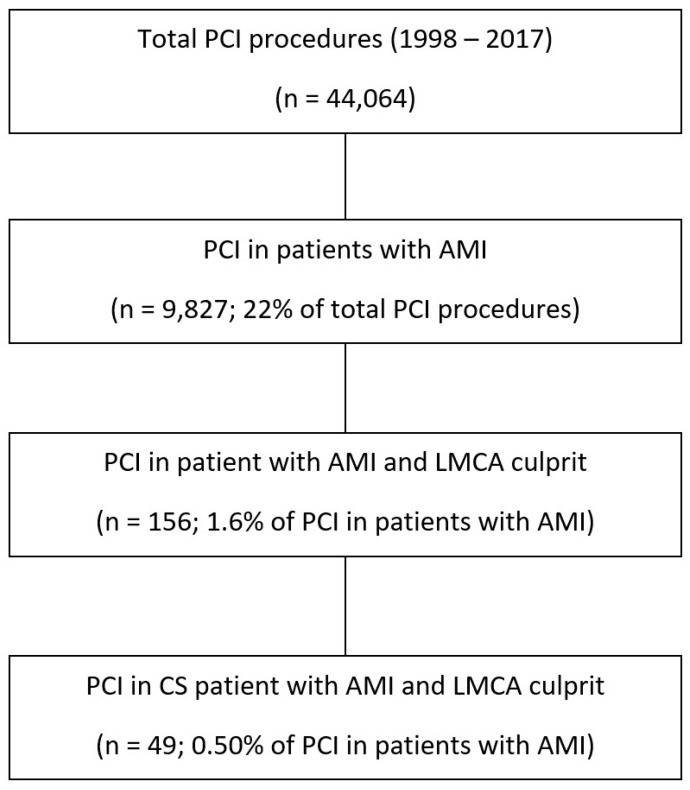
In this retrospective analysis, all consecutive patients undergoing PCI for cardiogenic shock secondary to total occlusive ULMCA-related AMI were included between January 1998 and January 2017. The primary endpoint was 30-day mortality. The secondary endpoints were long-term mortality and 30-day and long-term major adverse cardiovascular and cerebrovascular events. The differences in clinical and procedural variables were assessed. A multivariable model was created to search for independent predictors of survival.
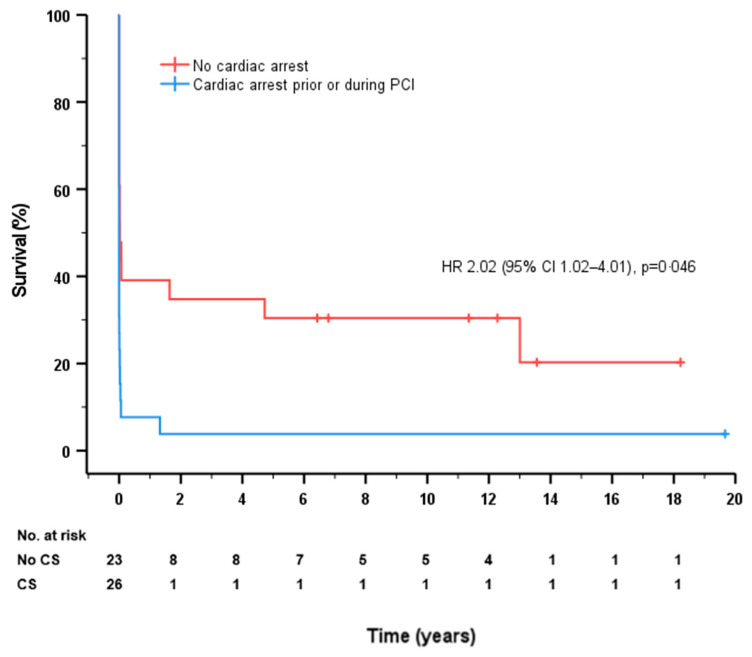
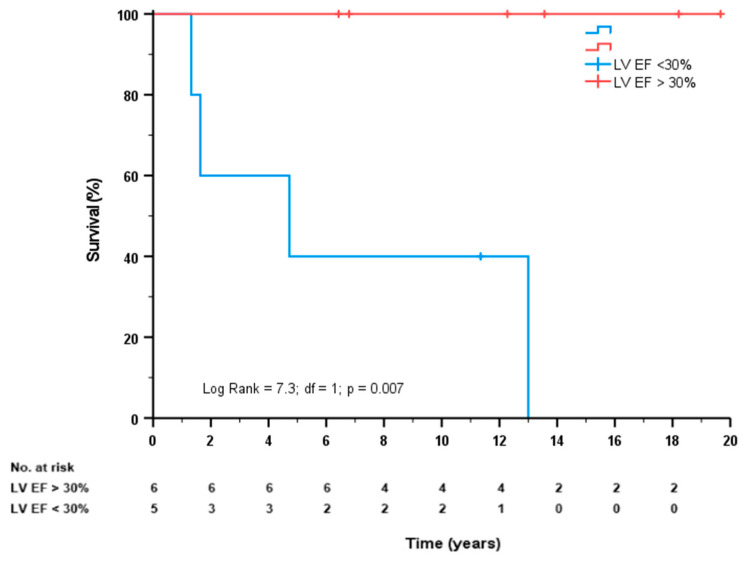
Forty-nine patients were included, and the mean age was 62 ± 11 years. The majority of patients suffered cardiac arrest prior or during PCI (51%). Thirty-day mortality was 78%, of which 55% died within 24 h. The median follow-up of patients who survived 30 days ( = 11) was 9.9 years (interquartile range 4.7-13.6), and long-term mortality was 84%. Long-term all-cause mortality was independently associated with cardiac arrest prior or during PCI (hazard ratio [HR] 2.02, 95% confidence interval 1.02-4.01, = 0.043). Patients who survived to the 30-day follow-up with severe left ventricular dysfunction had a significantly higher risk of mortality compared to patients with moderate to mild dysfunction ( = 0.007).
Cardiogenic shock secondary to total occlusive ULMCA-related AMI carries a very high 30-day all-cause mortality. Thirty-day survivors with a severe left ventricular dysfunction have a poor long-term prognosis.
急性心肌梗死(AMI)合并无保护左主干冠状动脉(ULMCA)闭塞是一种罕见疾病,死亡率很高。关于因ULMCA相关AMI继发心源性休克而行经皮冠状动脉介入治疗(PCI)后的临床结局的文献很少。
在这项回顾性分析中,纳入了1998年1月至2017年1月期间所有因ULMCA相关完全闭塞性AMI继发心源性休克而行PCI的连续患者。主要终点是30天死亡率。次要终点是长期死亡率以及30天和长期主要不良心血管和脑血管事件。评估了临床和手术变量的差异。建立了多变量模型以寻找生存的独立预测因素。
纳入49例患者,平均年龄为62±11岁。大多数患者在PCI之前或期间发生心脏骤停(51%)。30天死亡率为78%,其中55%在24小时内死亡。存活30天的患者(n = 11)的中位随访时间为9.9年(四分位间距4.7 - 13.6),长期死亡率为84%。长期全因死亡率与PCI之前或期间的心脏骤停独立相关(风险比[HR] 2.02,95%置信区间1.02 - 4.01,P = 0.043)。与中度至轻度功能障碍的患者相比,存活至30天随访且有严重左心室功能障碍的患者死亡率显著更高(P = 0.007)。
因ULMCA相关完全闭塞性AMI继发的心源性休克30天全因死亡率非常高。有严重左心室功能障碍的30天幸存者长期预后较差。