Department of Obstetrics and Prenatal Medicine, University Hospital Bonn, Venusberg Campus 1, 53127, Bonn, Germany.
Prenatal Care Dr. Marquet and Bewermeyer, Muffeter Weg 37, 52074, Aachen, Germany.
Arch Gynecol Obstet. 2024 Mar;309(3):987-992. doi: 10.1007/s00404-023-06970-5. Epub 2023 Feb 25.
Less than a dozen cases of psoas abscesses in pregnancy have been described in the literature. We reviewed the literature when treating a patient with a psoas abscess after ipsilateral double J-ureteral stent placement (in the following: "double J-stent") due to infected hydronephrosis.
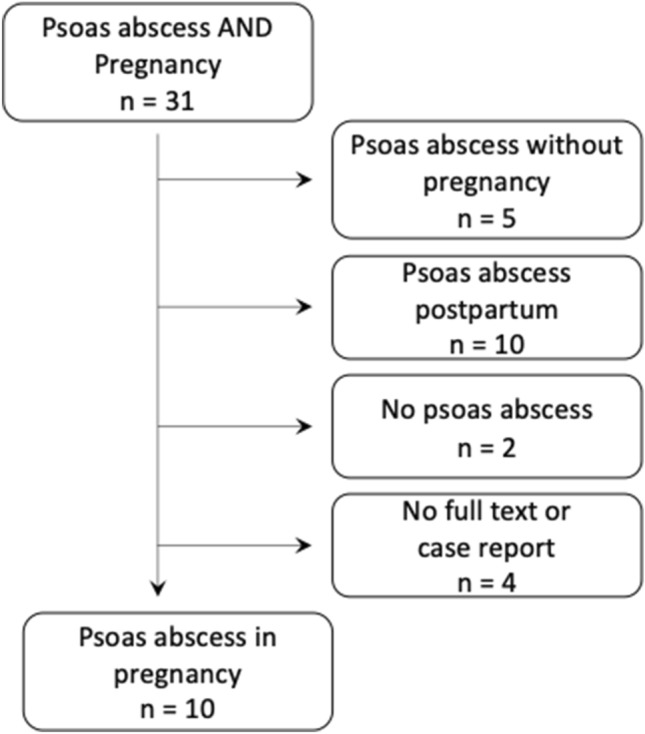
In January 2022, this review was searched using the Pubmed/MEDLINE database and the mesh terms "Psoas Abscess" AND "Pregnancy". Studies were included in any language and of all years, describing a psoas abscess during pregnancy. When patients did not have a psoas abscess, the abscess occurred after pregnancy, or when there was no full text available, the article was excluded.
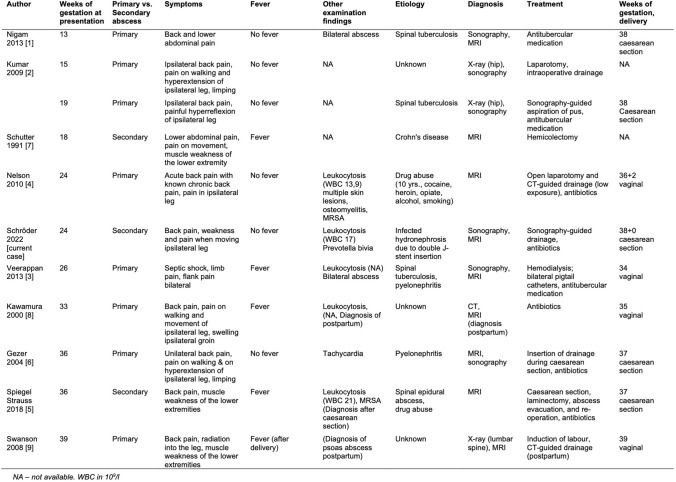
Ten case reports about patients with psoas abscesses during pregnancy were included. The classical symptomatic triad of psoas muscle abscess included lower back pain, limping and persistent fever with daily spikes. However, in most cases, not all three symptoms can be found. Especially, fever is absent in more than half of the patients. Psoas abscesses are described between 13 and 39 weeks of gestation. Primary psoas abscesses with haematogenous spread are more common during pregnancy than secondary with spread per continuitatem. In the literature, the main reasons for psoas abscess are spinal tuberculosis, drug abuse or underlying diseases such as Crohn's disease. It is not uncommon for the definite cause to be unclear. Regarding the patient's symptoms, pyelonephritis is often considered a possible aetiology. In general, the main treatment options include antibiotic treatment and abscess drainage. There is no higher caesarean section rate, and no negative outcome for the foetus has been described.
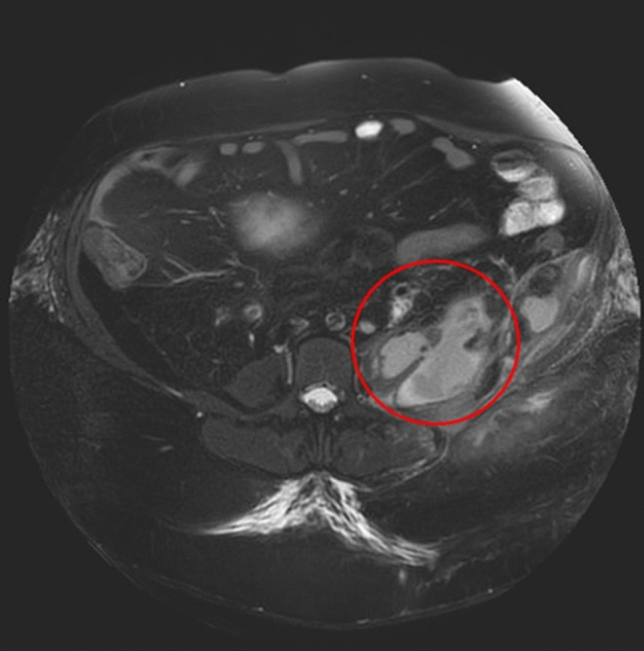
In our patient, a 38-year-old obese Caucasian woman, who had received a left double J-stent for infected hydronephrosis at 15 weeks of gestation, we successfully treated a psoas abscess of 20 × 10 cm with a sonographically assisted abscess drainage and antibiotics. The further course of pregnancy and the elective repeat caesarean section at 38 + 0 weeks of gestation were without any problems. Double J-stent placement and laser stone lithotripsy during puerperium were performed because of recurrent urolithiasis.
Although rare, psoas abscesses can occur during pregnancy, and it has often been treated surgically in the past. A psoas abscess as a complication after infected hydronephrosis and intervention during pregnancy has never been reported in the literature. Even for obese patients, minimally invasive therapy may be a treatment option that has rarely been reported in the literature.
文献中仅描述了十几例妊娠合并腰大肌脓肿病例。我们在治疗一名因感染性肾盂积水而接受同侧双 J 输尿管支架置入(以下简称“双 J 支架”)后发生腰大肌脓肿的患者时,回顾了文献。
2022 年 1 月,我们使用 Pubmed/MEDLINE 数据库和主题词“腰大肌脓肿”和“妊娠”进行了检索。纳入所有语言和所有年份描述妊娠期间发生腰大肌脓肿的研究。当患者没有腰大肌脓肿、脓肿发生在妊娠后或无法获取全文时,则排除该文章。
纳入了 10 例妊娠合并腰大肌脓肿患者的病例报告。腰大肌脓肿的典型三联征包括腰痛、跛行和持续发热,每日有高峰。然而,在大多数情况下,并非所有三种症状都能找到。特别是,超过一半的患者没有发热。腰大肌脓肿发生在妊娠 13 至 39 周之间。妊娠期间,血源性播散引起的原发性腰大肌脓肿比继发性经连续途径播散引起的更常见。在文献中,腰大肌脓肿的主要原因是脊柱结核、药物滥用或克罗恩病等潜在疾病。明确病因并不常见。关于患者的症状,肾盂肾炎常被认为是一种可能的病因。一般来说,主要的治疗选择包括抗生素治疗和脓肿引流。剖宫产率没有升高,也没有描述对胎儿产生不良后果。
在我们的患者中,一名 38 岁肥胖的白人女性,在妊娠 15 周时因感染性肾盂积水接受左侧双 J 支架置入,我们成功地通过超声引导下脓肿引流和抗生素治疗了一个 20×10cm 的腰大肌脓肿。妊娠的进一步过程和 38+0 周的选择性剖宫产均无任何问题。产后因复发性尿路结石行双 J 支架置入和激光碎石术。
尽管罕见,但妊娠期间可能会发生腰大肌脓肿,过去常需手术治疗。文献中从未报道过因感染性肾盂积水和妊娠期间介入而导致的腰大肌脓肿作为并发症。即使对于肥胖患者,微创治疗也可能是一种治疗选择,在文献中也很少有报道。