Simão André Lopes, Palma Carolina Santos, Izquierdo-Sanchez Laura, Putignano Antonella, Carvalho-Gomes Angela, Posch Andreas, Zanaga Paola, Girleanu Irina, Henrique Mariana Moura, Araújo Carlos, Degre Delphine, Gustot Thierry, Sahuco Iván, Spagnolo Elia, Carvalhana Sofia, Moura Miguel, Fernandes Diogo Ae, Banales Jesus M, Romero-Gomez Manuel, Trifan Anca, Russo Francesco Paolo, Stauber Rudolf, Berenguer Marina, Moreno Christophe, Gonçalves João, Cortez-Pinto Helena, Castro Rui E
Research Institute for Medicines (iMed.ULisboa), Faculty of Pharmacy, Universidade de Lisboa, Lisbon, Portugal.
Department of Liver and Gastrointestinal Diseases, Biodonostia Health Research Institute, Donostia University Hospital, University of the Basque Country (UPV/EHU), San Sebastian, Spain.
JHEP Rep. 2023 May;5(5):100697. doi: 10.1016/j.jhepr.2023.100697. Epub 2023 Feb 20.
BACKGROUND & AIMS: The response of patients with chronic liver disease (CLD) to COVID-19 vaccines remains unclear. Our aim was to assess the humoral immune response and efficacy of two-dose COVID-19 vaccines among patients with CLD of different aetiologies and disease stages.
A total of 357 patients were recruited in clinical centres from six European countries, and 132 healthy volunteers served as controls. Serum IgG (nM), IgM (nM), and neutralising antibodies (%) against the Wuhan-Hu-1, B.1.617, and B.1.1.529 SARS-CoV-2 spike proteins were determined before vaccination (T0) and 14 days (T2) and 6 months (T3) after the second-dose vaccination. Patients fulfilling inclusion criteria at T2 (n = 212) were stratified into 'low' or 'high' responders according to IgG levels. Infection rates and severity were collected throughout the study.
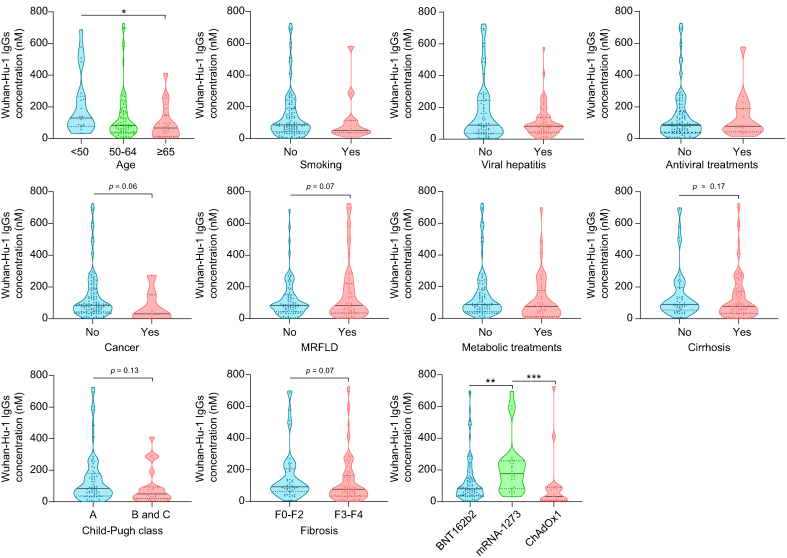
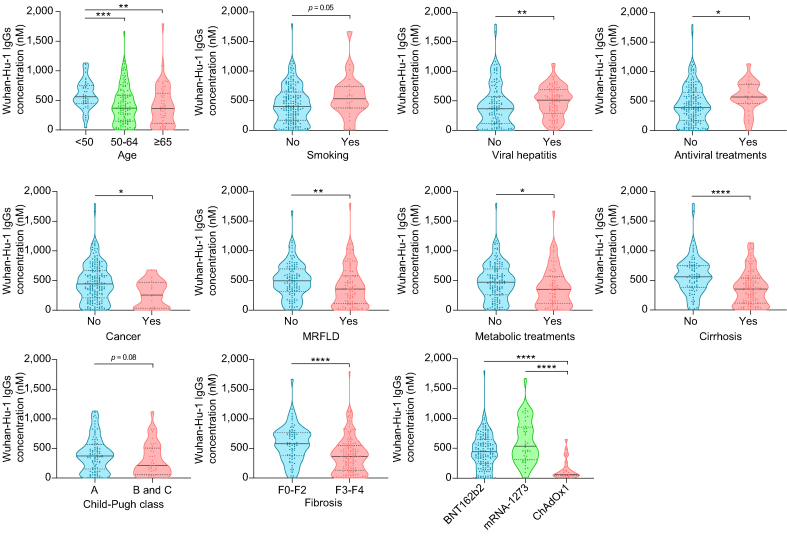
Wuhan-Hu-1 IgG, IgM, and neutralisation levels significantly increased from T0 to T2 in patients vaccinated with BNT162b2 (70.3%), mRNA-1273 (18.9%), or ChAdOx1 (10.8%). In multivariate analysis, age, cirrhosis, and type of vaccine (ChAdOx1 > BNT162b2 > mRNA-1273) predicted 'low' humoral response, whereas viral hepatitis and antiviral therapy predicted 'high' humoral response. Compared with Wuhan-Hu-1, B.1.617 and, further, B.1.1.529 IgG levels were significantly lower at both T2 and T3. Compared with healthy individuals, patients with CLD presented with lower B.1.1.529 IgGs at T2 with no additional key differences. No major clinical or immune IgG parameters associated with SARS-CoV-2 infection rates or vaccine efficacy.
Patients with CLD and cirrhosis exhibit lower immune responses to COVID-19 vaccination, irrespective of disease aetiology. The type of vaccine leads to different antibody responses that appear not to associate with distinct efficacy, although this needs validation in larger cohorts with a more balanced representation of all vaccines.
In patients with CLD vaccinated with two-dose vaccines, age, cirrhosis, and type of vaccine (Vaxzevria > Pfizer BioNTech > Moderna) predict a 'lower' humoral response, whereas viral hepatitis aetiology and prior antiviral therapy predict a 'higher' humoral response. This differential response appears not to associate with SARS-CoV-2 infection incidence or vaccine efficacy. However, compared with Wuhan-Hu-1, humoral immunity was lower for the Delta and Omicron variants, and all decreased after 6 months. As such, patients with CLD, particularly those older and with cirrhosis, should be prioritised for receiving booster doses and/or recently approved adapted vaccines.
慢性肝病(CLD)患者对新冠疫苗的反应尚不清楚。我们的目的是评估不同病因和疾病阶段的CLD患者中两剂新冠疫苗的体液免疫反应和疗效。
从六个欧洲国家的临床中心招募了357名患者,并选取132名健康志愿者作为对照。在接种疫苗前(T0)、第二剂疫苗接种后14天(T2)和6个月(T3)测定针对武汉-1、B.1.617和B.1.1.529 严重急性呼吸综合征冠状病毒2(SARS-CoV-2)刺突蛋白的血清IgG(纳摩尔)、IgM(纳摩尔)和中和抗体(%)。在T2时符合纳入标准的患者(n = 212)根据IgG水平分为“低”或“高”反应者。在整个研究过程中收集感染率和严重程度。
接种BNT162b2(70.3%)、mRNA-1273(18.9%)或ChAdOx1(10.8%)的患者中,武汉-1 IgG、IgM和中和水平从T0到T2显著升高。在多变量分析中,年龄、肝硬化和疫苗类型(ChAdOx1 > BNT162b2 > mRNA-1273)预测“低”体液反应,而病毒性肝炎和抗病毒治疗预测“高”体液反应。与武汉-1相比,B.1.617以及进一步的B.1.1.529 IgG水平在T2和T3时均显著较低。与健康个体相比,CLD患者在T2时B.1.1.529 IgGs较低,无其他关键差异。没有主要临床或免疫IgG参数与SARS-CoV-2感染率或疫苗疗效相关。
CLD和肝硬化患者对新冠疫苗的免疫反应较低,与疾病病因无关。疫苗类型导致不同的抗体反应,似乎与不同的疗效无关,尽管这需要在所有疫苗更均衡代表的更大队列中进行验证。
在接种两剂疫苗的CLD患者中,年龄、肝硬化和疫苗类型(Vaxzevria > 辉瑞BioNTech > 莫德纳)预测“较低”的体液反应,而病毒性肝炎病因和先前的抗病毒治疗预测“较高”的体液反应。这种差异反应似乎与SARS-CoV-2感染发生率或疫苗疗效无关。然而,与武汉-1相比,Delta和Omicron变体的体液免疫较低,且6个月后均下降。因此,CLD患者,特别是老年和肝硬化患者,应优先接受加强剂量和/或最近批准的适配疫苗。