Albon Dana, Zhang Lijia, Patrie James, Jones Marieke, Li Z Galvin, Noonan Emily, Borish Larry
Departments of Medicine, University of Virginia School of Medicine, 800546, Charlottesville, VA, 22908, USA.
Department of Psychiatry, Virginia Commonwealth University, Richmond, VA, USA.
Allergy Asthma Clin Immunol. 2023 Feb 27;19(1):15. doi: 10.1186/s13223-023-00760-z.
The Cystic Fibrosis Foundation Patient Registry (CFFPR) reports a high prevalence of asthma (34.6%) in people with Cystic Fibrosis (PwCF). While our current understanding of this relationship is limited, a type 2 inflammatory (T2) phenotype has often been identified in CF patients.
This study aimed to evaluate the relationship between the eosinophilic CF T2 inflammatory phenotype and CF-related pulmonary outcomes and microbiological data.
We conducted a retrospective chart review of adult patients with CF (18 and older; n = 93) receiving their care at University of Virginia Medical Center adult program from January, 2013 through December, 2018. Data collected included demographic data, CFTR (CF transmembrane conductance regulator) mutation, CF comorbidities, medications, Absolute Eosinophil Counts (AEC) in cells/µL and Immunoglobulin E (IgE) levels in IU/mL.
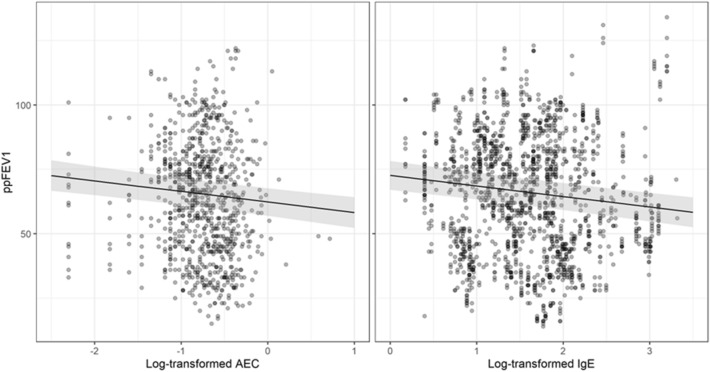
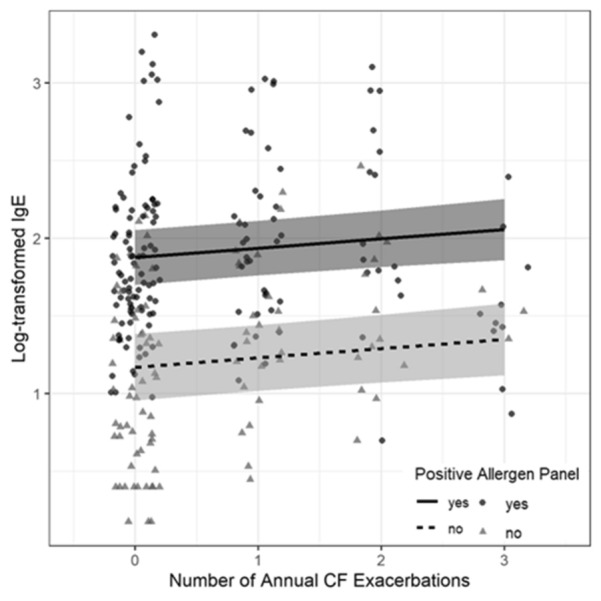
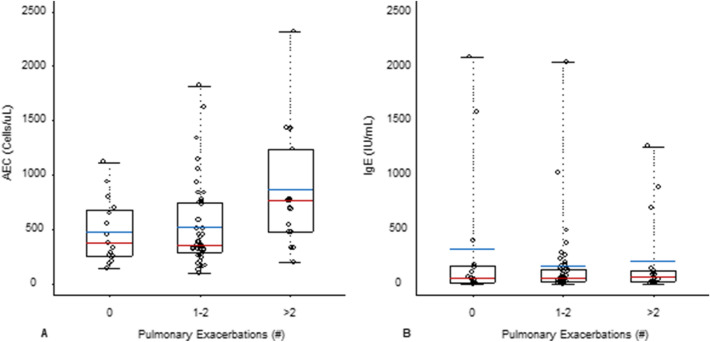
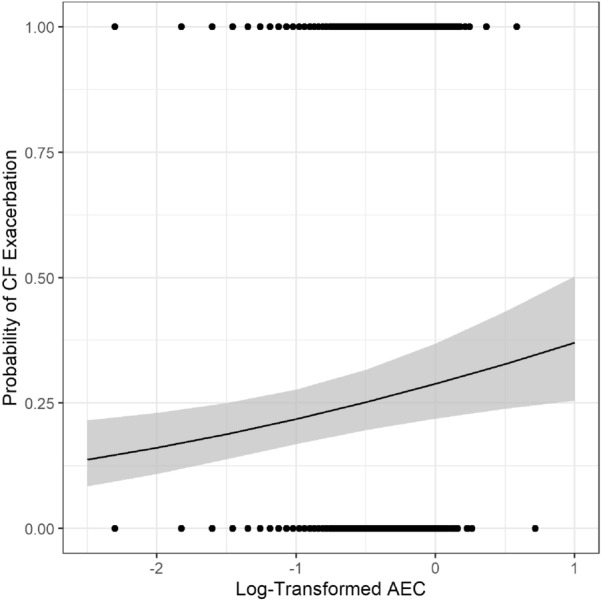
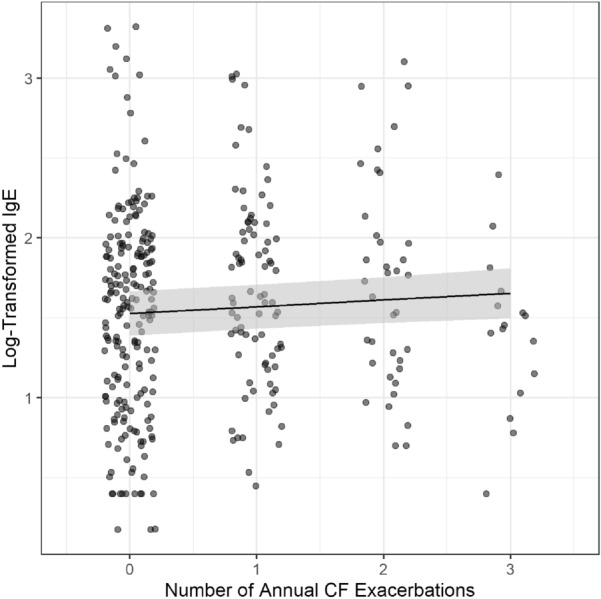
Of 93 patients screened for study eligibility, 74 were included in the final analysis; 19 patients were excluded due to lack of longitudinal data across the study timeline. Lung function decline correlated with increased AEC (p < 0.001) and IgE (p < 0.001) even when adjusting for covariates: age, gender, presence of Pseudomonas spp., MRSA, other bacterial spp., Aspergillus spp., and other fungi (p < 0.001). Univariate analysis demonstrated that people with CF who experienced more than 2 exacerbations requiring hospitalizations and/or intravenous antibiotics a year were more likely to have high AEC (p = 0.018). Logistic regression showed that as AEC increases, the probability that the measurement was taken during a CF exacerbation increases (p = 0.0039). A linear mixed model showed that each additional annual exacerbation event increased on average the log IgE by 0.04. (p = 0.015). This finding remained stable in a multivariate model (p = 0.0145). When adjusted for atopy, log IgE increases as the number of exacerbation events increases (p = 0.022). There was no association between AEC and IgE and microbiological colonization.
This study has shown that in CF patients, T2 inflammation based on serum AEC and IgE correlated with pulmonary exacerbations requiring hospitalizations and/or intravenous antibiotics, independent of bacterial airway colonization. In addition, lung function decline correlated with increased IgE and AEC. Further studies are needed to explore these correlations and potential impact on treatment.
囊性纤维化基金会患者登记处(CFFPR)报告称,囊性纤维化患者(PwCF)中哮喘的患病率很高(34.6%)。虽然我们目前对这种关系的了解有限,但在囊性纤维化患者中经常发现2型炎症(T2)表型。
本研究旨在评估嗜酸性囊性纤维化T2炎症表型与囊性纤维化相关的肺部结局及微生物学数据之间的关系。
我们对2013年1月至2018年12月在弗吉尼亚大学医学中心成人项目接受治疗的成年囊性纤维化患者(18岁及以上;n = 93)进行了回顾性病历审查。收集的数据包括人口统计学数据、CFTR(囊性纤维化跨膜传导调节因子)突变、囊性纤维化合并症、药物、每微升细胞中的绝对嗜酸性粒细胞计数(AEC)以及每毫升国际单位的免疫球蛋白E(IgE)水平。
在93名筛查符合研究资格的患者中,74名被纳入最终分析;19名患者因在整个研究时间范围内缺乏纵向数据而被排除。即使在调整协变量(年龄、性别、铜绿假单胞菌属、耐甲氧西林金黄色葡萄球菌、其他细菌属、曲霉属和其他真菌)后,肺功能下降仍与AEC升高(p < 0.001)和IgE升高(p < 0.001)相关(p < 0.001)。单因素分析表明,每年经历超过2次需要住院和/或静脉使用抗生素的加重发作的囊性纤维化患者更有可能具有高AEC(p = 0.018)。逻辑回归显示,随着AEC的增加,在囊性纤维化加重发作期间进行测量的概率增加(p = 0.0039)。线性混合模型显示,每年额外增加一次加重发作事件,平均使log IgE增加0.04(p = 0.015)。这一发现在多变量模型中保持稳定(p = 0.0145)。在调整特应性后,log IgE随着加重发作事件数量的增加而增加(p = 0.022)。AEC和IgE与微生物定植之间没有关联。
本研究表明,在囊性纤维化患者中,基于血清AEC和IgE的T2炎症与需要住院和/或静脉使用抗生素的肺部加重发作相关,与气道细菌定植无关。此外,肺功能下降与IgE和AEC升高相关。需要进一步研究来探索这些相关性及其对治疗的潜在影响。