Channon-Wells Samuel, Vito Ortensia, McArdle Andrew J, Seaby Eleanor G, Patel Harsita, Shah Priyen, Pazukhina Ekaterina, Wilson Clare, Broderick Claire, D'Souza Giselle, Keren Ilana, Nijman Ruud G, Tremoulet Adriana, Munblit Daniel, Ulloa-Gutierrez Rolando, Carter Michael J, Ramnarayan Padmanabhan, De Tisham, Hoggart Clive, Whittaker Elizabeth, Herberg Jethro A, Kaforou Myrsini, Cunnington Aubrey J, Blyuss Oleg, Levin Michael
Centre for Paediatrics and Child Health, Faculty of Medicine, Imperial College London, London, UK.
Department of Infectious Disease, Section of Paediatric Infectious Disease, Faculty of Medicine, Imperial College London, London, UK.
Lancet Rheumatol. 2023 Apr;5(4):e184-e199. doi: 10.1016/S2665-9913(23)00029-2. Epub 2023 Feb 14.
Multisystem inflammatory syndrome in children (MIS-C), a hyperinflammatory condition associated with SARS-CoV-2 infection, has emerged as a serious illness in children worldwide. Immunoglobulin or glucocorticoids, or both, are currently recommended treatments.
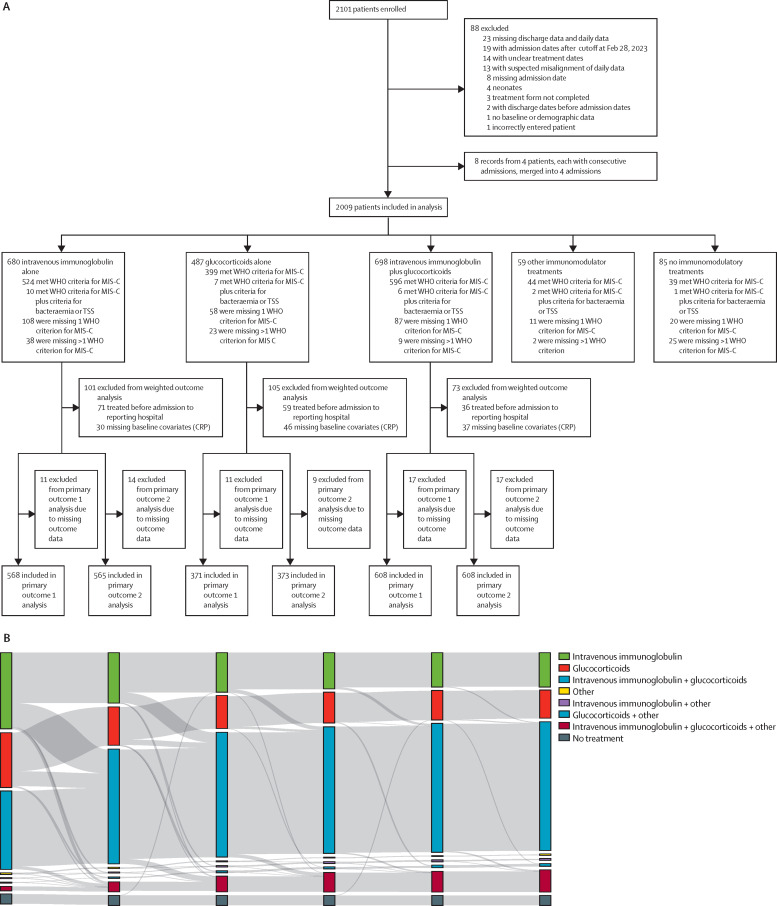
The Best Available Treatment Study evaluated immunomodulatory treatments for MIS-C in an international observational cohort. Analysis of the first 614 patients was previously reported. In this propensity-weighted cohort study, clinical and outcome data from children with suspected or proven MIS-C were collected onto a web-based Research Electronic Data Capture database. After excluding neonates and incomplete or duplicate records, inverse probability weighting was used to compare primary treatments with intravenous immunoglobulin, intravenous immunoglobulin plus glucocorticoids, or glucocorticoids alone, using intravenous immunoglobulin as the reference treatment. Primary outcomes were a composite of inotropic or ventilator support from the second day after treatment initiation, or death, and time to improvement on an ordinal clinical severity scale. Secondary outcomes included treatment escalation, clinical deterioration, fever, and coronary artery aneurysm occurrence and resolution. This study is registered with the ISRCTN registry, ISRCTN69546370.
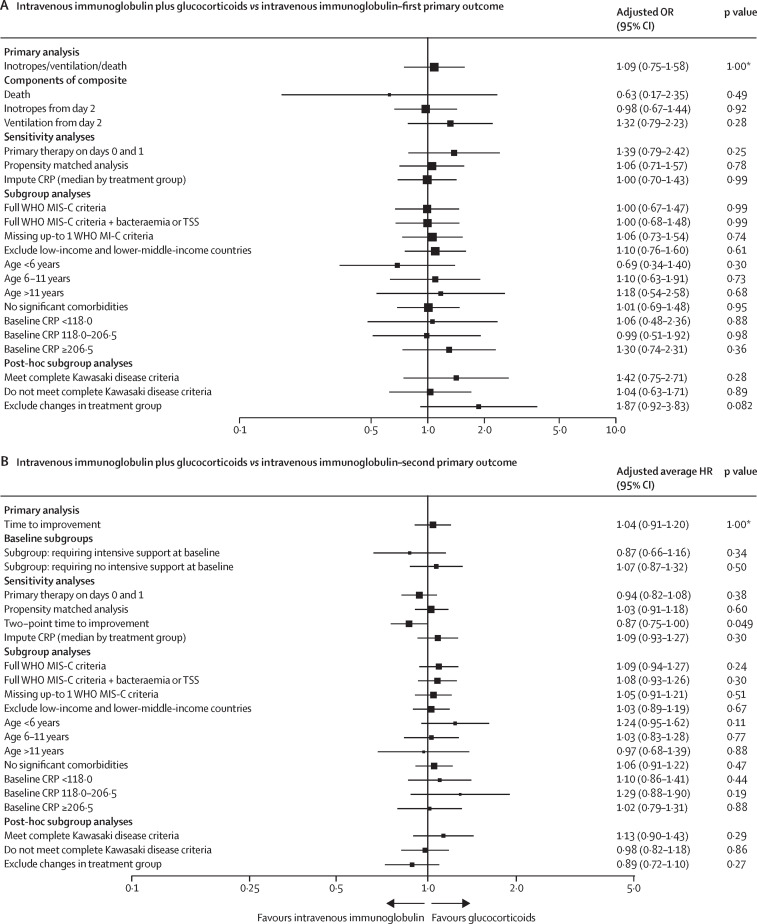
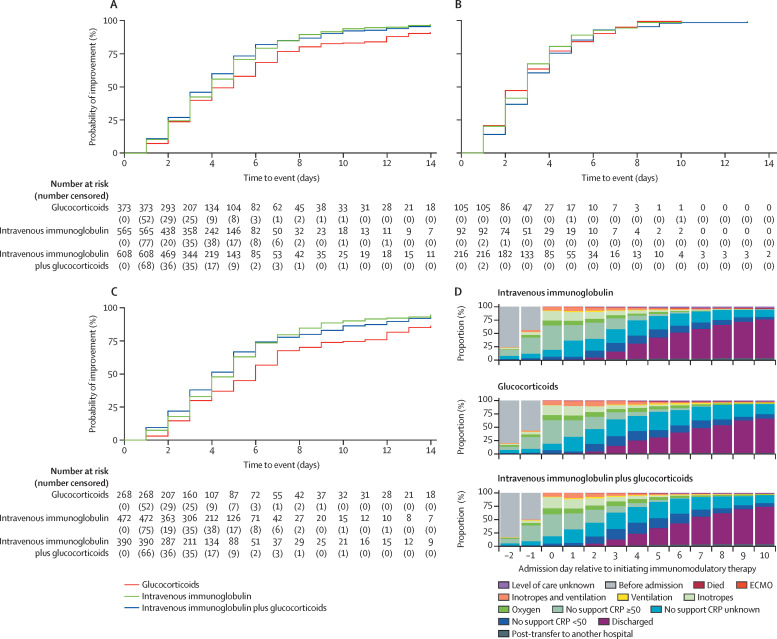
We enrolled 2101 children (aged 0 months to 19 years) with clinically diagnosed MIS-C from 39 countries between June 14, 2020, and April 25, 2022, and, following exclusions, 2009 patients were included for analysis (median age 8·0 years [IQR 4·2-11·4], 1191 [59·3%] male and 818 [40·7%] female, and 825 [41·1%] White). 680 (33·8%) patients received primary treatment with intravenous immunoglobulin, 698 (34·7%) with intravenous immunoglobulin plus glucocorticoids, 487 (24·2%) with glucocorticoids alone; 59 (2·9%) patients received other combinations, including biologicals, and 85 (4·2%) patients received no immunomodulators. There were no significant differences between treatments for primary outcomes for the 1586 patients with complete baseline and outcome data that were considered for primary analysis. Adjusted odds ratios for ventilation, inotropic support, or death were 1·09 (95% CI 0·75-1·58; corrected p value=1·00) for intravenous immunoglobulin plus glucocorticoids and 0·93 (0·58-1·47; corrected p value=1·00) for glucocorticoids alone, versus intravenous immunoglobulin alone. Adjusted average hazard ratios for time to improvement were 1·04 (95% CI 0·91-1·20; corrected p value=1·00) for intravenous immunoglobulin plus glucocorticoids, and 0·84 (0·70-1·00; corrected p value=0·22) for glucocorticoids alone, versus intravenous immunoglobulin alone. Treatment escalation was less frequent for intravenous immunoglobulin plus glucocorticoids (OR 0·15 [95% CI 0·11-0·20]; p<0·0001) and glucocorticoids alone (0·68 [0·50-0·93]; p=0·014) versus intravenous immunoglobulin alone. Persistent fever (from day 2 onward) was less common with intravenous immunoglobulin plus glucocorticoids compared with either intravenous immunoglobulin alone (OR 0·50 [95% CI 0·38-0·67]; p<0·0001) or glucocorticoids alone (0·63 [0·45-0·88]; p=0·0058). Coronary artery aneurysm occurrence and resolution did not differ significantly between treatment groups.
Recovery rates, including occurrence and resolution of coronary artery aneurysms, were similar for primary treatment with intravenous immunoglobulin when compared to glucocorticoids or intravenous immunoglobulin plus glucocorticoids. Initial treatment with glucocorticoids appears to be a safe alternative to immunoglobulin or combined therapy, and might be advantageous in view of the cost and limited availability of intravenous immunoglobulin in many countries.
Imperial College London, the European Union's Horizon 2020, Wellcome Trust, the Medical Research Foundation, UK National Institute for Health and Care Research, and National Institutes of Health.
儿童多系统炎症综合征(MIS-C)是一种与严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染相关的高炎症状态,已在全球范围内成为儿童的一种严重疾病。目前推荐使用免疫球蛋白或糖皮质激素,或两者联合进行治疗。
最佳可用治疗研究在一个国际观察性队列中评估了MIS-C的免疫调节治疗。先前已报告了对前614例患者的分析。在这项倾向加权队列研究中,将疑似或确诊为MIS-C的儿童的临床和结局数据收集到基于网络的研究电子数据采集数据库中。在排除新生儿以及不完整或重复的记录后,使用逆概率加权法,以静脉注射免疫球蛋白作为对照治疗,比较静脉注射免疫球蛋白、静脉注射免疫球蛋白加糖皮质激素或单独使用糖皮质激素的主要治疗方法。主要结局是治疗开始后第二天开始使用血管活性药物或呼吸机支持,或死亡的综合情况,以及在序数临床严重程度量表上改善的时间。次要结局包括治疗升级、临床恶化、发热以及冠状动脉瘤的发生和消退情况。本研究已在国际标准随机对照试验编号注册中心注册,编号为ISRCTN69546370。
我们纳入了2020年6月14日至2022年4月25日期间来自39个国家的2101名临床诊断为MIS-C的儿童(年龄从0个月至19岁),排除后,纳入2009例患者进行分析(中位年龄8.0岁[四分位间距4.2 - 11.4],男性1191例[59.3%],女性818例[40.7%],白人825例[41.1%])。680例(33.8%)患者接受静脉注射免疫球蛋白作为主要治疗,698例(34.7%)接受静脉注射免疫球蛋白加糖皮质激素,487例(24.2%)接受单独使用糖皮质激素;59例(2.9%)患者接受其他联合治疗,包括生物制剂,85例(4.2%)患者未接受免疫调节剂治疗。在1586例有完整基线和结局数据并纳入主要分析的患者中,各治疗组在主要结局方面无显著差异。与单独使用静脉注射免疫球蛋白相比,静脉注射免疫球蛋白加糖皮质激素的通气、血管活性药物支持或死亡的校正比值比为1.09(95%置信区间0.75 - 1.58;校正p值 = 1.00),单独使用糖皮质激素的校正比值比为0.93(0.58 - 1.47;校正p值 = 1.00)。与单独使用静脉注射免疫球蛋白相比,静脉注射免疫球蛋白加糖皮质激素改善时间的校正平均风险比为1.04(95%置信区间0.91 - 1.20;校正p值 = 1.00),单独使用糖皮质激素的校正平均风险比为0.84(0.70 - 1.00;校正p值 = 0.22)。与单独使用静脉注射免疫球蛋白相比,静脉注射免疫球蛋白加糖皮质激素(比值比0.15[95%置信区间0.11 - 0.20];p < 0.0001)和单独使用糖皮质激素(0.68[0.50 - 0.93];p = 0.014)治疗升级的频率较低。与单独使用静脉注射免疫球蛋白(比值比0.50[95%置信区间0.38 - 0.67];p < 0.0001)或单独使用糖皮质激素(0.63[0.45 - 0.88];p = 0.0058)相比,静脉注射免疫球蛋白加糖皮质激素持续发热(从第2天起)的情况较少见。各治疗组冠状动脉瘤的发生和消退情况无显著差异。
与糖皮质激素或静脉注射免疫球蛋白加糖皮质激素相比,静脉注射免疫球蛋白作为主要治疗的恢复率,包括冠状动脉瘤的发生和消退情况相似。糖皮质激素初始治疗似乎是免疫球蛋白或联合治疗的一种安全替代方案,鉴于许多国家静脉注射免疫球蛋白的成本和供应有限,可能具有优势。
伦敦帝国学院、欧盟地平线2020计划、惠康信托基金会、医学研究基金会、英国国家健康与照护研究机构以及美国国立卫生研究院。