Division of Hematology/Oncology, David Geffen School of Medicine at UCLA, Santa Monica, USA.
Department of Radiology, David Geffen School of Medicine at UCLA, Santa Monica, USA.
ESMO Open. 2023 Apr;8(2):100884. doi: 10.1016/j.esmoop.2023.100884. Epub 2023 Feb 28.
Talimogene laherparepvec (T-VEC), a first-in-class oncolytic viral immunotherapy, enhances tumor-specific immune activation. T-VEC combined with atezolizumab, which blocks inhibitor T-cell checkpoints, could provide greater benefit than either agent alone. Safety/efficacy of the combination was explored in patients with triple negative breast cancer (TNBC) or colorectal cancer (CRC) with liver metastases.
In this phase Ib, multicenter, open-label, parallel cohort study of adults with TNBC or CRC with liver metastases, T-VEC (10 then 10 PFU/ml; ≤4 ml) was administered into hepatic lesions via image-guided injection every 21 (±3) days. Atezolizumab 1200 mg was given on day 1 and every 21 (±3) days thereafter. Treatment continued until patients experienced dose-limiting toxicity (DLT), had complete response, progressive disease, needed alternative anticancer treatment, or withdrew due to an adverse event (AE). The primary endpoint was DLT incidence, and secondary endpoints included efficacy and AEs.
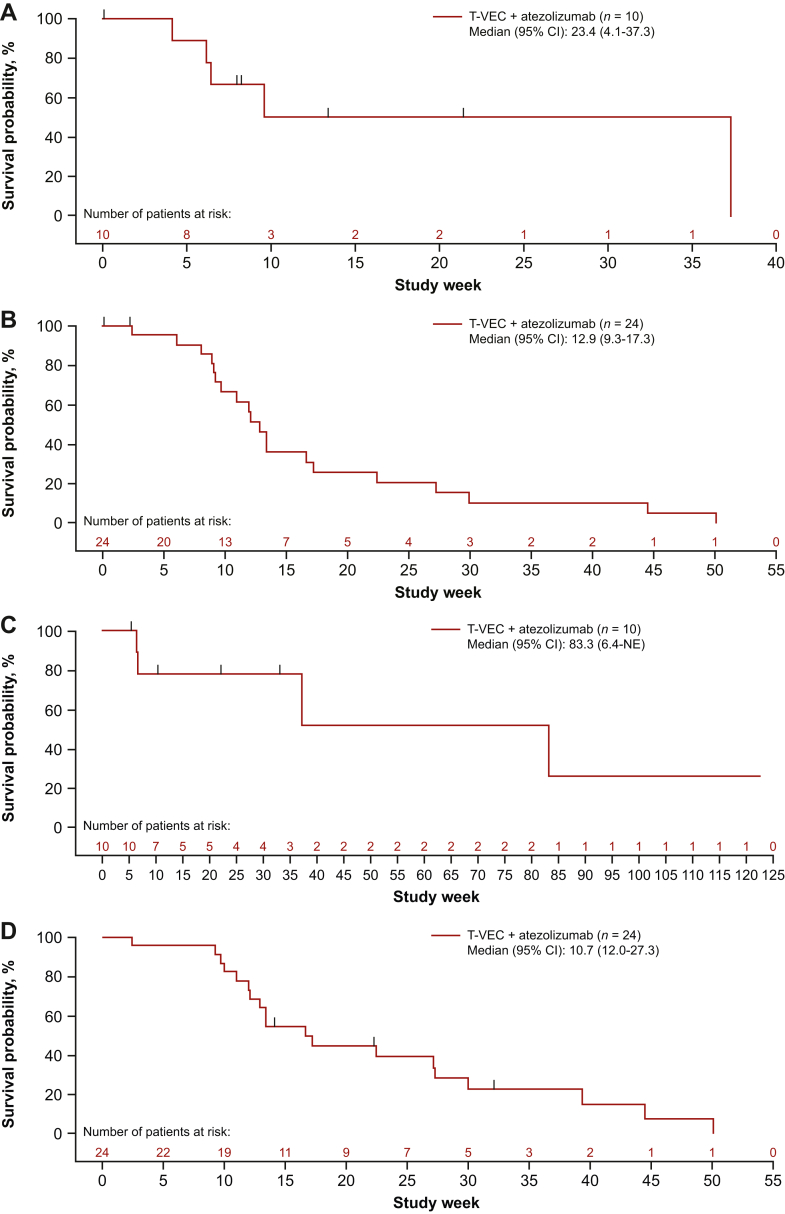
Between 19 March 2018 and 6 November 2020, 11 patients with TNBC were enrolled (safety analysis set: n = 10); between 19 March 2018 and 16 October 2019, 25 patients with CRC were enrolled (safety analysis set: n = 24). For the 5 patients in the TNBC DLT analysis set, no patient had DLT; for the 18 patients in the CRC DLT analysis set, 3 (17%) had DLT, all serious AEs. AEs were reported by 9 (90%) TNBC and 23 (96%) CRC patients, the majority with grade ≥3 [TNBC, 7 (70%); CRC, 13 (54%)], and 1 was fatal [CRC, 1 (4%)]. Evidence of efficacy was limited. Overall response rate was 10% (95% confidence interval 0.3-44.5) for TNBC; one (10%) patient had a partial response. For CRC, no patients had a response; 14 (58%) were unassessable.
The safety profile reflected known risks with T-VEC including risks of intrahepatic injection; no unexpected safety findings from addition of atezolizumab to T-VEC were observed. Limited evidence of antitumor activity was observed.
Talimogene laherparepvec(T-VEC)是一种首创的溶瘤病毒免疫疗法,可增强肿瘤特异性免疫激活。T-VEC 联合可阻断抑制性 T 细胞检查点的阿替利珠单抗,可能比单独使用任何一种药物更有效。在患有三阴性乳腺癌(TNBC)或结直肠癌(CRC)伴肝转移的患者中,对联合用药的安全性/疗效进行了探索。
这是一项在成人 TNBC 或 CRC 伴肝转移患者中开展的、多中心、开放标签、平行队列的 Ib 期研究,对肝内病变进行影像学引导下注射 T-VEC(10 次和 10 PFU/ml;≤4ml),每 21(±3)天一次。阿替利珠单抗 1200mg 在第 1 天给予,此后每 21(±3)天一次。治疗持续至患者出现剂量限制性毒性(DLT)、完全缓解、疾病进展、需要替代抗癌治疗或因不良事件(AE)而退出。主要终点是 DLT 发生率,次要终点包括疗效和 AE。
在 2018 年 3 月 19 日至 2020 年 11 月 6 日期间,共纳入了 11 例 TNBC 患者(安全性分析集:n=10);在 2018 年 3 月 19 日至 2019 年 10 月 16 日期间,共纳入了 25 例 CRC 患者(安全性分析集:n=24)。在 TNBC DLT 分析集的 5 例患者中,无患者发生 DLT;在 CRC DLT 分析集的 18 例患者中,3 例(17%)发生 DLT,均为严重 AE。9 例(90%)TNBC 患者和 23 例(96%)CRC 患者报告了 AE,大多数为≥3 级(TNBC:7[70%];CRC:13[54%]),1 例为致命性(CRC:1[4%])。疗效证据有限。TNBC 的总缓解率为 10%(95%置信区间 0.3-44.5),1 例(10%)患者有部分缓解。CRC 患者无缓解,14 例(58%)无法评估。
安全性特征反映了 T-VEC 已知风险,包括肝内注射风险;未观察到阿替利珠单抗联合 T-VEC 治疗的意外安全性发现。观察到有限的抗肿瘤活性证据。