Australian Centre for Health Services Innovation, Queensland University of Technology, Brisbane, Queensland, Australia.
Department of Respiratory & Sleep Medicine, Queensland Children's Hospital, Brisbane, Queensland, Australia.
Respirology. 2023 Apr;28(4):339-349. doi: 10.1111/resp.14479. Epub 2023 Mar 2.
This position statement, updated from the 2015 guidelines for managing Australian and New Zealand children/adolescents and adults with chronic suppurative lung disease (CSLD) and bronchiectasis, resulted from systematic literature searches by a multi-disciplinary team that included consumers. The main statements are: Diagnose CSLD and bronchiectasis early; this requires awareness of bronchiectasis symptoms and its co-existence with other respiratory diseases (e.g., asthma, chronic obstructive pulmonary disease). Confirm bronchiectasis with a chest computed-tomography scan, using age-appropriate protocols and criteria in children. Undertake a baseline panel of investigations. Assess baseline severity, and health impact, and develop individualized management plans that include a multi-disciplinary approach and coordinated care between healthcare providers. Employ intensive treatment to improve symptom control, reduce exacerbation frequency, preserve lung function, optimize quality-of-life and enhance survival. In children, treatment also aims to optimize lung growth and, when possible, reverse bronchiectasis. Individualize airway clearance techniques (ACTs) taught by respiratory physiotherapists, encourage regular exercise, optimize nutrition, avoid air pollutants and administer vaccines following national schedules. Treat exacerbations with 14-day antibiotic courses based upon lower airway culture results, local antibiotic susceptibility patterns, clinical severity and patient tolerance. Patients with severe exacerbations and/or not responding to outpatient therapy are hospitalized for further treatments, including intravenous antibiotics and intensive ACTs. Eradicate Pseudomonas aeruginosa when newly detected in lower airway cultures. Individualize therapy for long-term antibiotics, inhaled corticosteroids, bronchodilators and mucoactive agents. Ensure ongoing care with 6-monthly monitoring for complications and co-morbidities. Undertake optimal care of under-served peoples, and despite its challenges, delivering best-practice treatment remains the overriding aim.
本立场声明是对澳大利亚和新西兰儿童/青少年及成人慢性化脓性肺疾病(CSLD)和支气管扩张症管理指南(2015 年版)的更新,由一个多学科团队进行了系统的文献检索,其中包括患者代表。主要声明如下:
尽早诊断 CSLD 和支气管扩张症;这需要认识到支气管扩张症的症状及其与其他呼吸系统疾病(如哮喘、慢性阻塞性肺疾病)的共存。
在儿童中,使用适合年龄的方案和标准,通过胸部计算机断层扫描(CT)扫描来确认支气管扩张症。
进行基线检查。评估基线严重程度和健康影响,并制定个体化的管理计划,包括多学科方法和医疗保健提供者之间的协调护理。
采用强化治疗以改善症状控制、减少恶化频率、保持肺功能、优化生活质量并提高生存率。在儿童中,治疗还旨在优化肺生长,并在可能的情况下逆转支气管扩张症。
由呼吸理疗师教授个体化气道清除技术(ACTs),鼓励定期锻炼、优化营养、避免空气污染物,并按照国家计划接种疫苗。
根据下呼吸道培养结果、当地抗生素药敏模式、临床严重程度和患者耐受性,用 14 天疗程的抗生素治疗恶化。
对于严重恶化和/或不能接受门诊治疗的患者,应住院进行进一步治疗,包括静脉内抗生素和强化 ACTs。
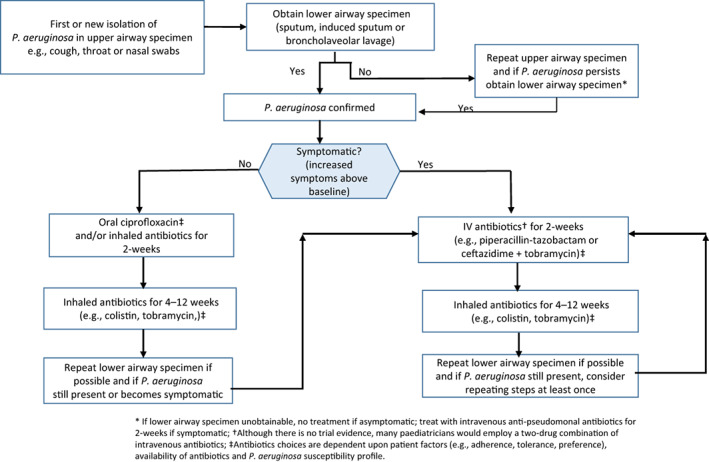
在下呼吸道培养中发现新的铜绿假单胞菌时,应进行个体化治疗。
个体化治疗长期抗生素、吸入性皮质类固醇、支气管扩张剂和黏液溶解剂。
确保通过每 6 个月的监测来进行并发症和合并症的持续护理。
为服务不足的人群提供最佳护理,尽管存在挑战,但提供最佳实践治疗仍然是首要目标。