Virginia Tech Carilion School of Medicine, Roanoke, VA, United States.
University Hospital at University of Virginia Medical Center, Charlottesville, VA, United States.
PeerJ. 2023 Feb 27;11:e14879. doi: 10.7717/peerj.14879. eCollection 2023.
Chronic kidney disease (CKD) poses a major public health burden. Diabetes mellitus (DM) is one of the major causes of CKD. In patients with DM, it can be difficult to differentiate diabetic kidney disease (DKD) from other causes of glomerular damage; it should not be assumed that all DM patients with decreased eGFR and/or proteinuria have DKD. Renal biopsy is the standard for definitive diagnosis, but other less invasive methods may provide clinical benefit. As previously reported, Raman spectroscopy of CKD patient urine with statistical and chemometric modeling may provide a novel, non-invasive methodology for discriminating between renal pathologies.
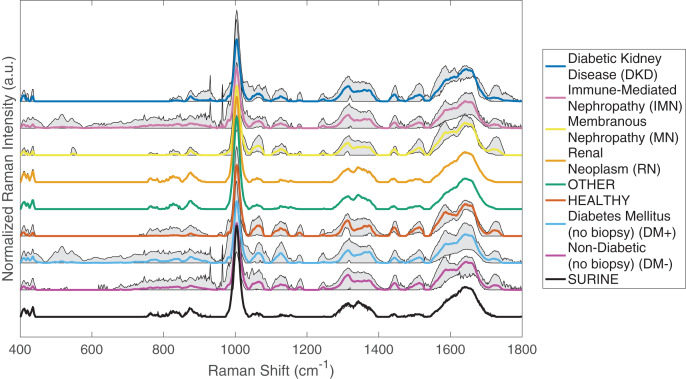
Urine samples were collected from renal biopsied and non-biopsied patients presenting with CKD secondary to DM and non-diabetic kidney disease. Samples were analyzed by Raman spectroscopy, baselined with the ISREA algorithm, and subjected to chemometric modeling. Leave-one-out cross-validation was used to assess the predictive capabilities of the model.
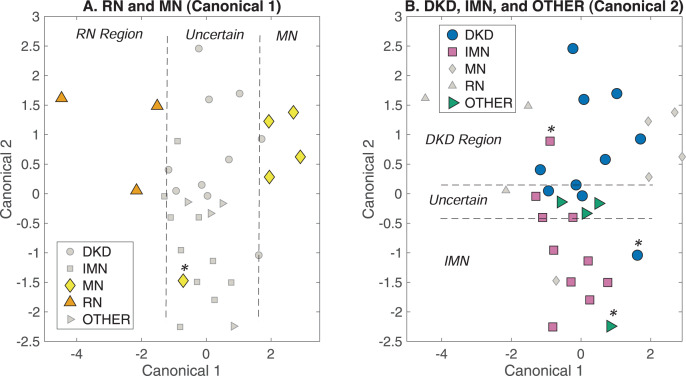
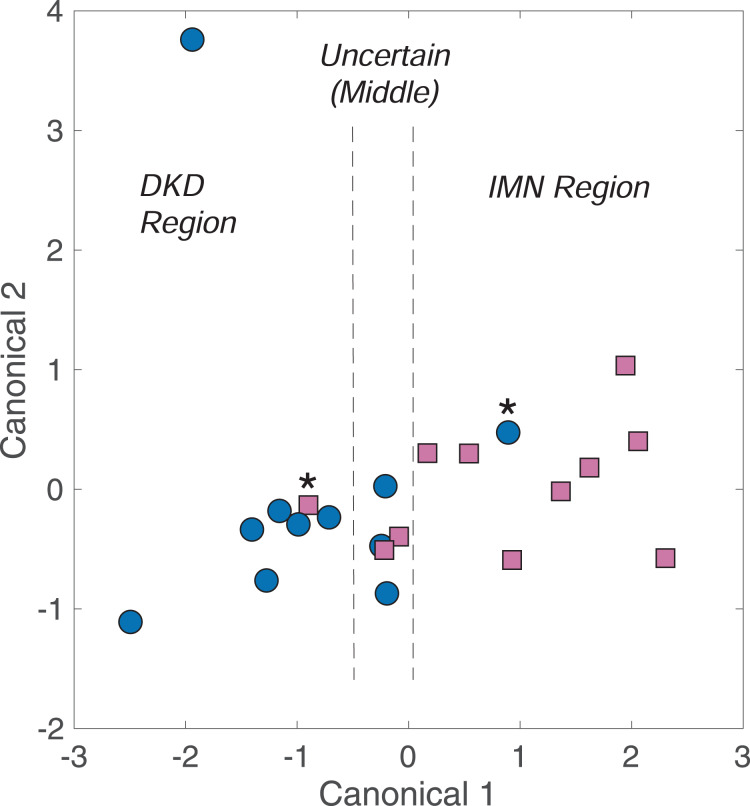
This proof-of-concept study consisted of 263 samples, including renal biopsied, non-biopsied diabetic and non-diabetic CKD patients, healthy volunteers, and the Surine™ urinalysis control. Urine samples of DKD patients and those with immune-mediated nephropathy (IMN) were distinguished from one another with 82% sensitivity, specificity, positive-predictive value (PPV), and negative-predictive value (NPV). Among urine samples from all biopsied CKD patients, renal neoplasia was identified in urine with 100% sensitivity, specificity, PPV, and NPV, and membranous nephropathy was identified with 66.7% sensitivity, 96.4% specificity, 80.0% PPV, and 93.1% NPV. Finally, DKD was identified among a population of 150 patient urine samples containing biopsy-confirmed DKD, other biopsy-confirmed glomerular pathologies, un-biopsied non-diabetic CKD patients (no DKD), healthy volunteers, and Surine™ with 36.4% sensitivity, 97.8% specificity, 57.1% PPV, and 95.1% NPV. The model was used to screen un-biopsied diabetic CKD patients and identified DKD in more than 8% of this population. IMN in diabetic patients was identified among a similarly sized and diverse population with 83.3% sensitivity, 97.7% specificity, 62.5% PPV, and 99.2% NPV. Finally, IMN in non-diabetic patients was identified with 50.0% sensitivity, 99.4% specificity, 75.0% PPV, and 98.3% NPV.
Raman spectroscopy of urine with chemometric analysis may be able to differentiate between DKD, IMN, and other glomerular diseases. Future work will further characterize CKD stages and glomerular pathology, while assessing and controlling for differences in factors such as comorbidities, disease severity, and other lab parameters.
慢性肾脏病(CKD)是一个主要的公共卫生负担。糖尿病(DM)是 CKD 的主要原因之一。在 DM 患者中,很难将糖尿病肾病(DKD)与其他肾小球损伤原因区分开来;不应假设所有 eGFR 降低和/或蛋白尿的 DM 患者都患有 DKD。肾活检是明确诊断的标准,但其他微创方法可能具有临床益处。如前所述,用统计和化学计量建模对 CKD 患者尿液进行拉曼光谱分析可能为区分肾脏病变提供一种新颖的、非侵入性的方法。
从患有 DM 和非糖尿病性肾脏疾病的 CKD 继发的肾活检和非肾活检患者中收集尿液样本。对样本进行拉曼光谱分析,用 ISREA 算法进行基线处理,并进行化学计量建模。采用留一法交叉验证评估模型的预测能力。
本概念验证研究共纳入 263 例样本,包括肾活检、非肾活检的 DM 和非 DM CKD 患者、健康志愿者和 Surine™尿液分析对照。DKD 患者和免疫介导性肾病(IMN)患者的尿液样本之间的区分具有 82%的敏感性、特异性、阳性预测值(PPV)和阴性预测值(NPV)。在所有肾活检 CKD 患者的尿液样本中,肾肿瘤的识别率为 100%,敏感性、特异性、PPV 和 NPV 均为 100%,膜性肾病的识别率为 66.7%,特异性为 96.4%,PPV 为 80.0%,NPV 为 93.1%。最后,在包含活检证实的 DKD、其他活检证实的肾小球病变、未经活检的非糖尿病性 CKD 患者(无 DKD)、健康志愿者和 Surine™的 150 例患者尿液样本中,使用该模型识别 DKD,其敏感性为 36.4%,特异性为 97.8%,PPV 为 57.1%,NPV 为 95.1%。该模型用于筛选未经活检的糖尿病性 CKD 患者,在该人群中发现超过 8%的患者患有 DKD。在同样大小和多样化的糖尿病患者中,IMN 的识别率为 83.3%,特异性为 97.7%,PPV 为 62.5%,NPV 为 99.2%。最后,在非糖尿病患者中,IMN 的识别率为 50.0%,特异性为 99.4%,PPV 为 75.0%,NPV 为 98.3%。
尿液的拉曼光谱分析结合化学计量分析可能能够区分 DKD、IMN 和其他肾小球疾病。未来的工作将进一步描述 CKD 分期和肾小球病理,同时评估和控制合并症、疾病严重程度和其他实验室参数等因素的差异。