Epidemic Intelligence Service Centers for Disease Control and Prevention Atlanta Georgia USA.
COVID-19 Emergency Response Team Centers for Disease Control and Prevention Atlanta Georgia USA.
Influenza Other Respir Viruses. 2023 Mar 2;17(3):e13107. doi: 10.1111/irv.13107. eCollection 2023 Mar.
Bacterial and viral infections can occur with SARS-CoV-2 infection, but prevalence, risk factors, and associated clinical outcomes are not fully understood.
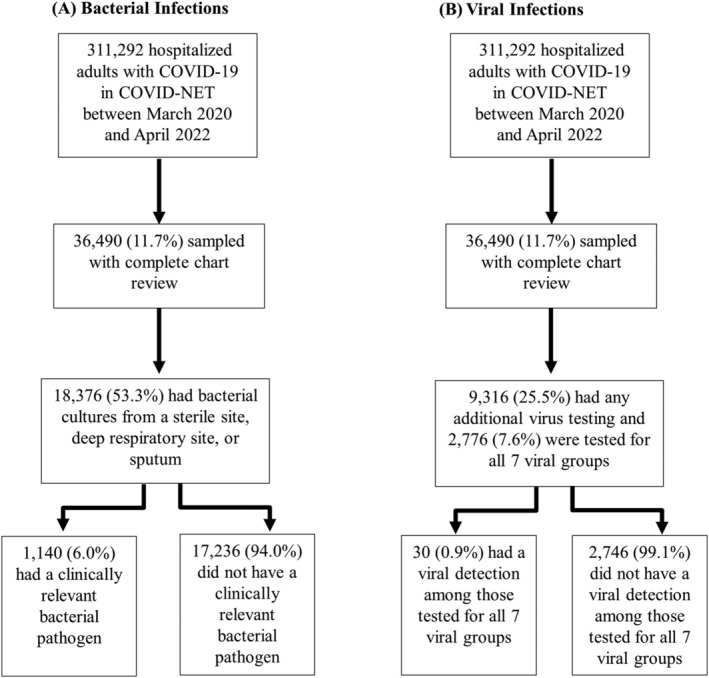
We used the Coronavirus Disease 2019-Associated Hospitalization Surveillance Network (COVID-NET), a population-based surveillance system, to investigate the occurrence of bacterial and viral infections among hospitalized adults with laboratory-confirmed SARS-CoV-2 infection between March 2020 and April 2022. Clinician-driven testing for bacterial pathogens from sputum, deep respiratory, and sterile sites were included. The demographic and clinical features of those with and without bacterial infections were compared. We also describe the prevalence of viral pathogens including respiratory syncytial virus, rhinovirus/enterovirus, influenza, adenovirus, human metapneumovirus, parainfluenza viruses, and non-SARS-CoV-2 endemic coronaviruses.
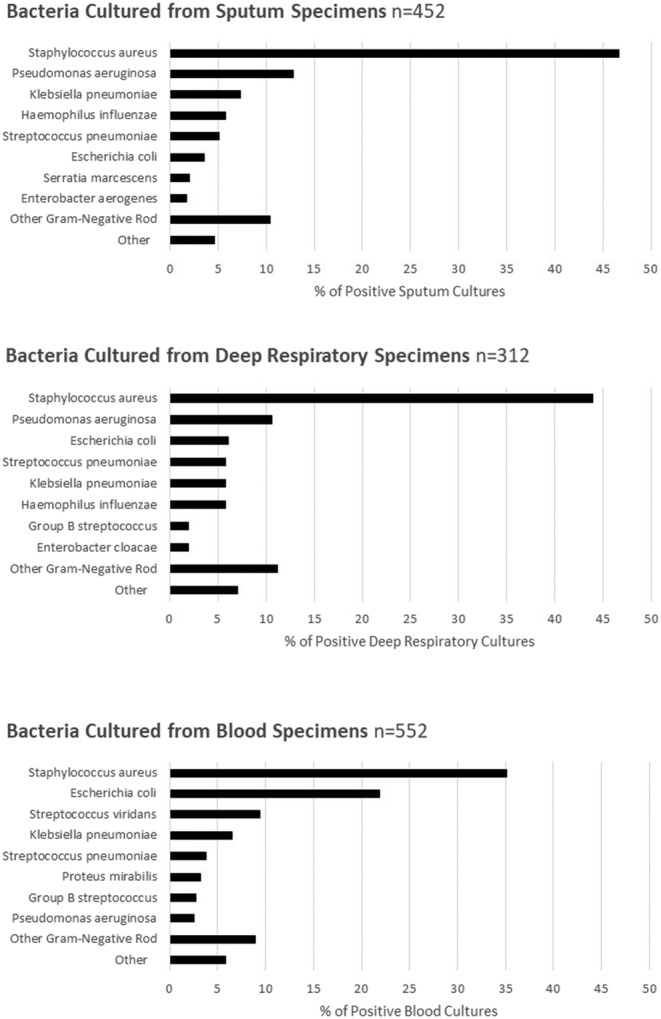
Among 36 490 hospitalized adults with COVID-19, 53.3% had bacterial cultures taken within 7 days of admission and 6.0% of these had a clinically relevant bacterial pathogen. After adjustment for demographic factors and co-morbidities, bacterial infections in patients with COVID-19 within 7 days of admission were associated with an adjusted relative risk of death 2.3 times that of patients with negative bacterial testing. and Gram-negative rods were the most frequently isolated bacterial pathogens. Among hospitalized adults with COVID-19, 2766 (7.6%) were tested for seven virus groups. A non-SARS-CoV-2 virus was identified in 0.9% of tested patients.
Among patients with clinician-driven testing, 6.0% of adults hospitalized with COVID-19 were identified to have bacterial coinfections and 0.9% were identified to have viral coinfections; identification of a bacterial coinfection within 7 days of admission was associated with increased mortality.
SARS-CoV-2 感染可并发细菌和病毒感染,但这些感染的流行情况、风险因素及相关临床结局尚不完全清楚。
我们利用基于人群的监测系统 2019 年冠状病毒病相关住院监测网络(COVID-NET),调查 2020 年 3 月至 2022 年 4 月期间实验室确诊 SARS-CoV-2 感染住院成人并发细菌和病毒感染的发生情况。纳入了来自痰、深部呼吸道和无菌部位的临床医生驱动的细菌病原体检测。比较了有和无细菌感染患者的人口统计学和临床特征。还描述了包括呼吸道合胞病毒、鼻病毒/肠病毒、流感、腺病毒、人偏肺病毒、副流感病毒和非 SARS-CoV-2 地方性冠状病毒在内的病毒病原体的流行情况。
在 36490 例 COVID-19 住院成人中,53.3%的患者在入院后 7 天内进行了细菌培养,其中 6.0%的患者有临床相关的细菌病原体。在调整了人口统计学因素和合并症后,COVID-19 患者在入院后 7 天内发生细菌感染与阴性细菌检测患者相比,死亡的调整相对风险增加 2.3 倍。革兰氏阳性球菌和革兰氏阴性杆菌是最常分离到的细菌病原体。在 COVID-19 住院成人中,766 例(7.6%)检测了 7 组病毒。在接受检测的患者中,有 0.9%的患者鉴定出非 SARS-CoV-2 病毒。
在有临床医生驱动检测的患者中,6.0%的 COVID-19 住院成人被鉴定为并发细菌感染,0.9%的患者被鉴定为并发病毒感染;入院后 7 天内鉴定出细菌合并感染与死亡率增加相关。