From the Department of Radiology, The First Affiliated Hospital of Fujian Medical University.
J Comput Assist Tomogr. 2023;47(4):539-547. doi: 10.1097/RCT.0000000000001448. Epub 2023 Mar 6.
This study aimed to explore the predictive performance of diffusion-weighted imaging with apparent diffusion coefficient map in predicting the proliferation rate of hepatocellular carcinoma and to develop a radiomics-based nomogram.
This was a single-center retrospective study. A total of 110 patients were enrolled. The sample included 38 patients with low Ki67 expression (Ki67 ≤10%) and 72 with high Ki67 expression (Ki67 >10%) as demonstrated by surgical pathology. Patients were randomly divided into either a training (n = 77) or validation (n = 33) cohort. Diffusion-weighted imaging with apparent diffusion coefficient maps was used to extract radiomic features and the signal intensity values of tumor (SI tumor ), normal liver (SI liver ), and background noise (SI background ) from all samples. Subsequently, the clinical model, radiomic model, and fusion model (with clinical data and radiomic signature) were developed and validated.
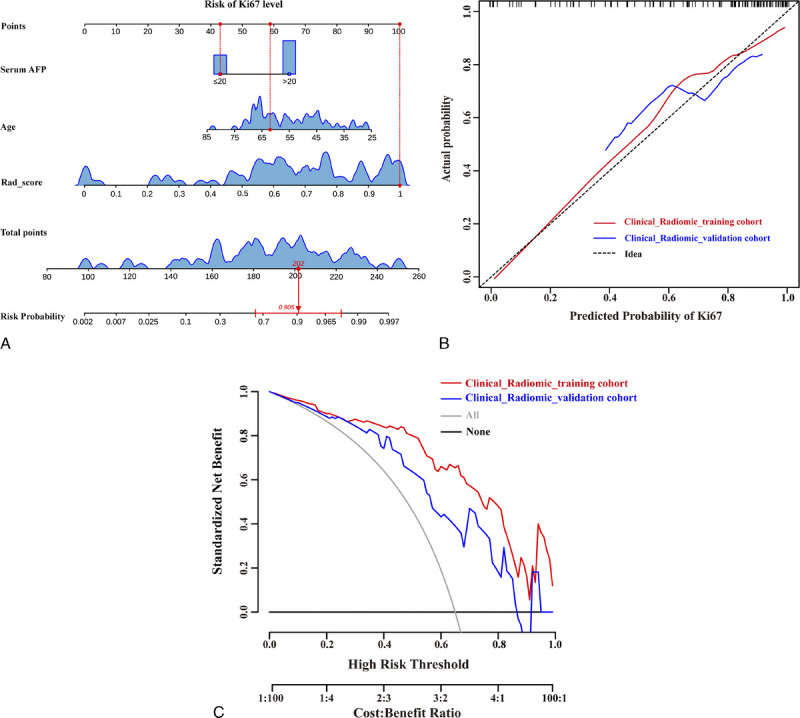
The area under the curve (AUC) of the clinical model for predicting the Ki67 expression including serum α-fetoprotein level ( P = 0.010), age ( P = 0.015), and signal noise ratio ( P = 0.026) was 0.799 and 0.715 in training and validation cohorts, respectively. The AUC of the radiomic model constructed by 9 selected radiomic features was 0.833 and 0.772 in training and validation cohorts, respectively. The AUC of the fusion model containing serum α-fetoprotein level ( P = 0.011), age ( P = 0.019), and rad score ( P < 0.001) was 0.901 and 0.781 in training and validation cohorts, respectively.
Diffusion-weighted imaging as a quantitative imaging biomarker can predict Ki67 expression level in hepatocellular carcinoma across various models.
本研究旨在探讨表观扩散系数图弥散加权成像对肝细胞癌增殖率的预测性能,并建立基于放射组学的列线图。
这是一项单中心回顾性研究。共纳入 110 例患者。样本包括 38 例 Ki67 低表达(Ki67≤10%)患者和 72 例 Ki67 高表达(Ki67>10%)患者,均经手术病理证实。患者被随机分为训练集(n=77)和验证集(n=33)。所有样本均采用弥散加权成像表观扩散系数图提取放射组学特征和肿瘤(SI 肿瘤)、正常肝(SI 肝)和背景噪声(SI 背景)的信号强度值。随后,建立并验证了临床模型、放射组学模型和融合模型(结合临床数据和放射组学特征)。
Ki67 表达预测的临床模型(包括血清甲胎蛋白水平(P=0.010)、年龄(P=0.015)和信号噪声比(P=0.026))的曲线下面积(AUC)在训练和验证组中分别为 0.799 和 0.715。由 9 个选定的放射组学特征构建的放射组学模型的 AUC 在训练和验证组中分别为 0.833 和 0.772。包含血清甲胎蛋白水平(P=0.011)、年龄(P=0.019)和 rad 评分(P<0.001)的融合模型的 AUC 在训练和验证组中分别为 0.901 和 0.781。
弥散加权成像作为一种定量成像生物标志物,可以在不同模型中预测肝细胞癌的 Ki67 表达水平。