Pinet Sandra, Durand Stéphanie, Perani Alexandre, Darnaud Léa, Amadjikpe Fifame, Yon Mathieu, Darbas Tiffany, Vergnenegre Alain, Egenod Thomas, Simonneau Yannick, Le Brun-Ly Valérie, Pestre Julia, Venat Laurence, Thuillier Frédéric, Chaunavel Alain, Duchesne Mathilde, Fermeaux Véronique, Guyot Anne, Lacorre Sylvain, Bessette Barbara, Lalloué Fabrice, Durand Karine, Deluche Elise
Medical Oncology Department, Dupuytren University Hospital, Limoges, France.
The National Institute for Health and Medical Research (INSERM) U1308 - CAPTuR "Control Of Cell Activation, Tumor Progression and Therapeutic Resistance", Faculty of Medicine, University of Limoges, Limoges, France.
Front Oncol. 2023 Feb 27;13:1104659. doi: 10.3389/fonc.2023.1104659. eCollection 2023.
In the context of personalized medicine, screening patients to identify targetable molecular alterations is essential for therapeutic decisions such as inclusion in clinical trials, early access to therapies, or compassionate treatment. The objective of this study was to determine the real-world impact of routine incorporation of FoundationOne analysis in cancers with a poor prognosis and limited treatment options, or in those progressing after at least one course of standard therapy.
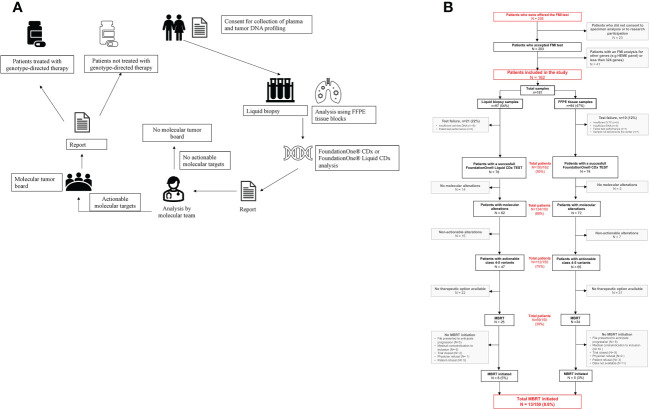
A FoundationOneCDx panel for solid tumor or liquid biopsy samples was offered to 204 eligible patients.
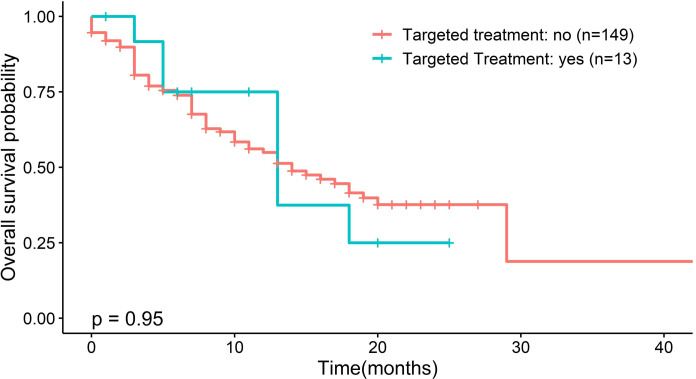
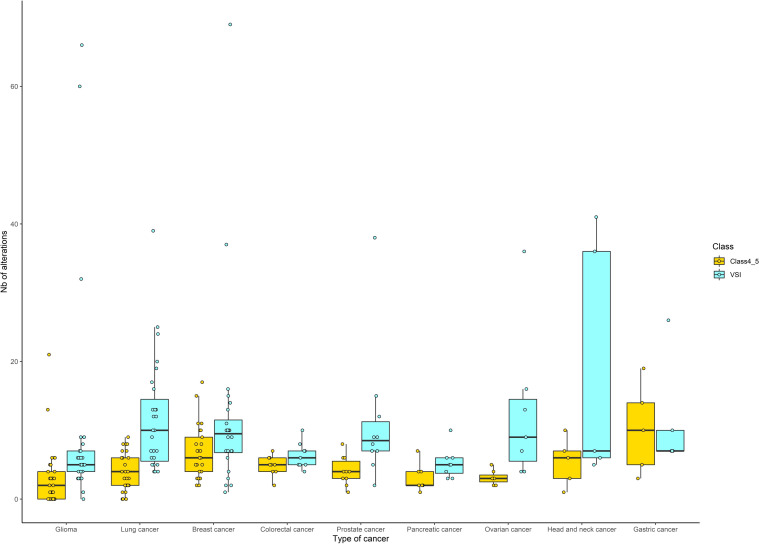
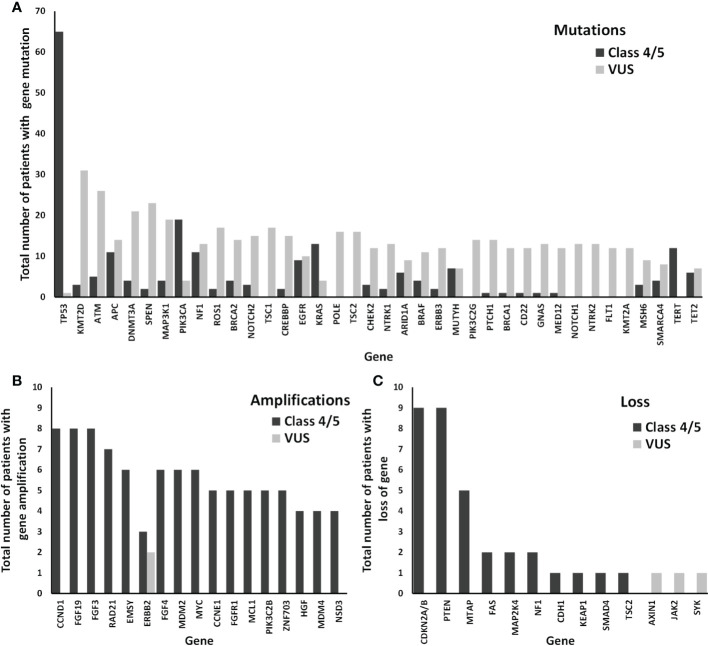
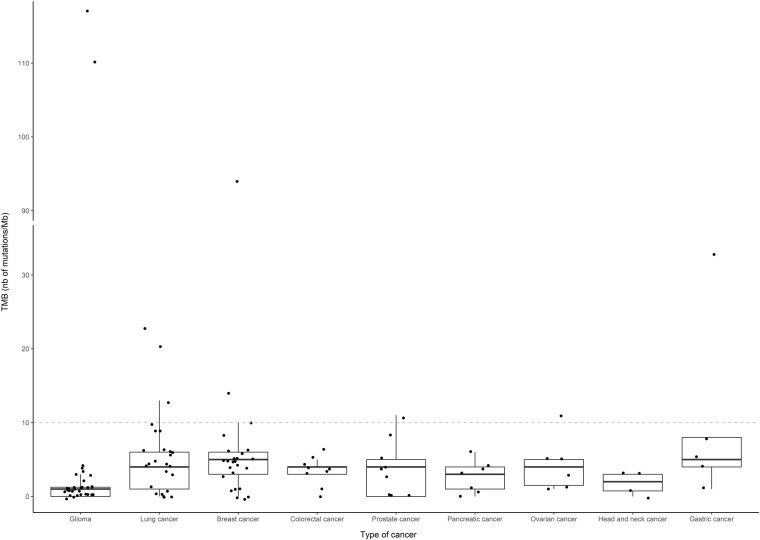
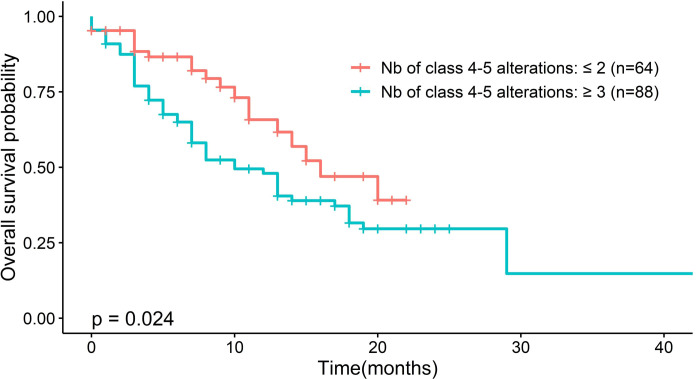
Samples from 150 patients were processed for genomic testing, with a data acquisition success rate of 93%. The analysis identified 2419 gene alterations, with a median of 11 alterations per tumor (range, 0-86). The most common or likely pathogenic variants were on , , , , , , , , and . The median tumor mutation burden was three mutations/Mb (range, 0-117) in 143 patients with available data. Of 150 patients with known or likely pathogenic actionable alterations, 13 (8.6%) received matched targeted therapy. Sixty-nine patients underwent Molecular Tumor Board, which resulted in recommendations in 60 cases. Treatment with genotype-directed therapy had no impact on overall survival (13 months 14 months; p = 0.95; hazard ratio = 1.04 (95% confidence interval, 0.48-2.26)].
This study highlights that an organized center with a Multidisciplinary Molecular Tumor Board and an NGS screening system can obtain satisfactory results comparable with those of large centers for including patients in clinical trials.
在精准医学背景下,筛查患者以确定可靶向的分子改变对于治疗决策至关重要,例如纳入临床试验、提前获得治疗或接受同情用药治疗。本研究的目的是确定在预后较差且治疗选择有限的癌症患者中,或在至少接受一个疗程标准治疗后病情进展的患者中,常规纳入FoundationOne分析的实际影响。
为204名符合条件的患者提供了用于实体瘤或液体活检样本的FoundationOneCDx检测。
对150名患者的样本进行了基因组检测,数据采集成功率为93%。分析确定了2419个基因改变,每个肿瘤的改变中位数为11个(范围为0 - 86)。最常见或可能致病的变异位于 、 、 、 、 、 、 、 、 和 。在143名有可用数据的患者中,肿瘤突变负荷中位数为3个突变/Mb(范围为0 - 117)。在150名已知或可能有致病可操作改变的患者中,13名(8.6%)接受了匹配的靶向治疗。69名患者接受了分子肿瘤学委员会评估,其中60例得出了建议。基因型导向治疗对总生存期无影响(13个月对14个月;p = 0.95;风险比 = 1.04(95%置信区间,0.48 - 2.26))。
本研究强调,一个拥有多学科分子肿瘤学委员会和二代测序筛查系统的有组织的中心,在将患者纳入临床试验方面能够获得与大型中心相当的满意结果。