Madjar Katrin, Mohindra Rajat, Durán-Pacheco Gonzalo, Rasul Rashad, Essioux Laurent, Maiya Vidya, Chandler G Scott
Product Development (PD), F. Hoffmann-La Roche, Basel, Switzerland.
Statistical Programming and Technology, Bristol Myers Squibb, Basel, Switzerland.
Front Oncol. 2023 Feb 28;13:1138305. doi: 10.3389/fonc.2023.1138305. eCollection 2023.
Immune checkpoint inhibitors (ICIs) have revolutionized the treatment of cancer patients in the last decade, but immune-related adverse events (irAEs) pose significant clinical challenges. Despite advances in the management of these unique toxicities, there remains an unmet need to further characterize the patient-level drivers of irAEs in order to optimize the benefit/risk balance in patients receiving cancer immunotherapy.
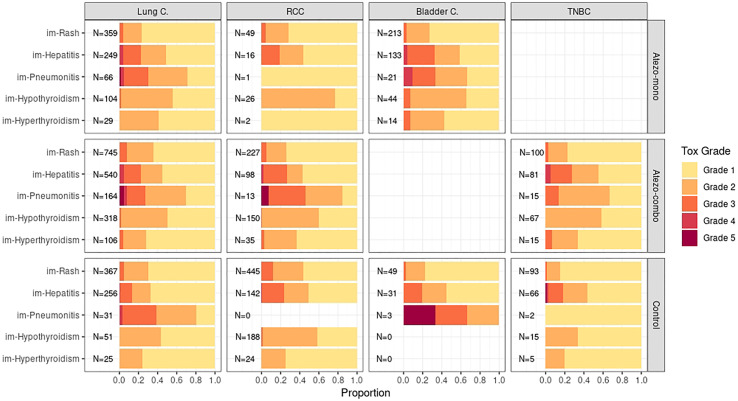
An individual-patient data meta-analysis was performed using data from 10,344 patients across 15 Roche sponsored clinical trials with atezolizumab in five different solid tumor types to assess the association between baseline risk factors and the time to onset of irAE. In this study, the overall analysis was conducted by treatment arm, indication, toxicity grade and irAE type, and the study design considered confounder adjustment to assess potential differences in risk factor profiles.
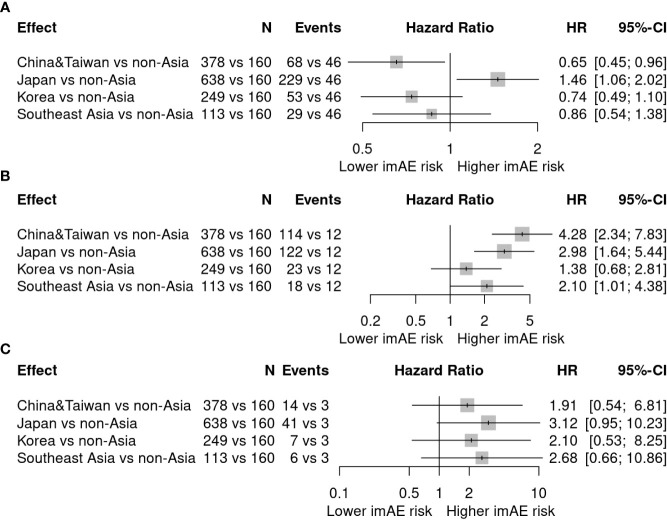
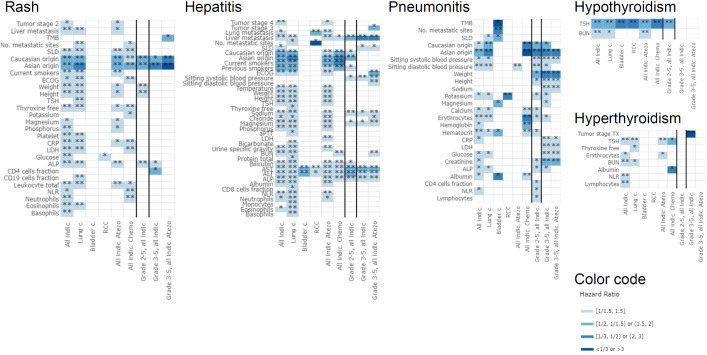
This analysis demonstrates that the safety profile of atezolizumab is generally consistent across indications in the 15 studies evaluated. In addition, our findings corroborate with prior reviews which suggest that reported rates of irAEs with PD-(L)1 inhibitors are nominally lower than CTLA-4 inhibitors. In our analysis, there were no remarkable differences in the distribution of toxicity grades between indications, but some indication-specific differences regarding the type of irAE were seen across treatment arms, where pneumonitis mainly occurred in lung cancer, and hypothyroidism and rash had a higher prevalence in advanced renal cell carcinoma compared to all other indications. Results showed consistency of risk factors across indications and by toxicity grade. The strongest and most consistent risk factors were mostly organ-specific such as elevated liver enzymes for hepatitis and thyroid stimulating hormone (TSH) for thyroid toxicities. Another strong but non-organ-specific risk factor was ethnicity, which was associated with rash, hepatitis and pneumonitis. Further understanding the impact of ethnicity on ICI associated irAEs is considered as an area for future research.
Overall, this analysis demonstrated that atezolizumab safety profile is consistent across indications, is clinically distinguishable from comparator regimens without checkpoint inhibition, and in line with literature, seems to suggest a nominally lower reported rates of irAEs vs CTLA-4 inhibitors. This analysis demonstrates several risk factors for irAEs by indication, severity and location of irAE, and by patient ethnicity. Additionally, several potential irAE risk factors that have been published to date, such as demographic factors, liver enzymes, TSH and blood cell counts, are assessed in this large-scale meta-analysis, providing a more consistent picture of their relevance. However, given the small effects size, changes to clinical management of irAEs associated with the use of Anti-PDL1 therapy are not warranted.
免疫检查点抑制剂(ICI)在过去十年中彻底改变了癌症患者的治疗方式,但免疫相关不良事件(irAE)带来了重大的临床挑战。尽管在管理这些独特毒性方面取得了进展,但仍有未满足的需求,需要进一步明确患者层面irAE的驱动因素,以优化接受癌症免疫治疗患者的获益/风险平衡。
利用来自罗氏公司赞助的15项临床试验中10344例患者的数据进行个体患者数据荟萃分析,这些试验涉及阿替利珠单抗治疗五种不同实体瘤类型,以评估基线风险因素与irAE发病时间之间的关联。在本研究中,总体分析按治疗组、适应证、毒性分级和irAE类型进行,研究设计考虑了混杂因素调整,以评估风险因素分布的潜在差异。
该分析表明,在评估的15项研究中,阿替利珠单抗的安全性概况在各适应证中总体一致。此外,我们的研究结果与先前的综述一致,该综述表明,报告的PD-(L)1抑制剂的irAE发生率名义上低于CTLA-4抑制剂。在我们的分析中,各适应证之间毒性分级的分布没有显著差异,但在各治疗组中观察到一些关于irAE类型的适应证特异性差异,其中肺炎主要发生在肺癌中,与所有其他适应证相比,甲状腺功能减退和皮疹在晚期肾细胞癌中的患病率更高。结果显示各适应证和毒性分级的风险因素具有一致性。最强且最一致的风险因素大多是器官特异性的,如肝炎时肝酶升高以及甲状腺毒性时促甲状腺激素(TSH)升高。另一个强烈但非器官特异性的风险因素是种族,它与皮疹、肝炎和肺炎相关。进一步了解种族对ICI相关irAE的影响被视为未来研究的一个领域。
总体而言,该分析表明阿替利珠单抗的安全性概况在各适应证中是一致的,在临床上与无检查点抑制的对照方案有区别,并且与文献一致,似乎表明报告的irAE发生率名义上低于CTLA-4抑制剂。该分析按适应证、irAE的严重程度和部位以及患者种族展示了几种irAE的风险因素。此外,在这项大规模荟萃分析中评估了一些迄今已发表的潜在irAE风险因素,如人口统计学因素、肝酶、TSH和血细胞计数,更一致地呈现了它们的相关性。然而,鉴于效应量较小,不建议改变与使用抗PDL1疗法相关的irAE的临床管理。