Habib Gul, Mahmood Khalid, Ahmad Latif, Gul Haji, Hayat Azam, Ur Rehman Mujaddad
Department of Microbiology, Abbottabad University of Science and Technology, Havelian Abbottabad, Pakistan.
National Institute of Virology, Dr. Panjwani Center for Molecular Medicine and Drug Research, International Center for Chemical and Biological Sciences, University of Karachi, Karachi, Pakistan.
J Clin Tuberc Other Mycobact Dis. 2023 May;31:100359. doi: 10.1016/j.jctube.2023.100359. Epub 2023 Mar 5.
The coronavirus 2019 pandemic was caused by a new single-strand RNA virus that originated from Wuhan, China, and infected more than 190 countries. The severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) coinfection with tuberculosis posed a serious public health concern and complicated the prognosis and treatment of patients. Since both are respiratory diseases, the sign and symptoms may overlap and could have synergistic effects on the host that can increase mortality during coinfection. The present investigation reported the clinical characteristics of patients having coinfection of COVID-19 and tuberculosis (COVID-TB).
We performed a retrospective investigation on COVID-19 infection in tuberculosis patients between the years 2020 and 2021. The SARS-CoV-2 was confirmed by PCR and the COVID-TB epidemiological and clinical findings were recorded on the day of admission and followed up for 25 days.
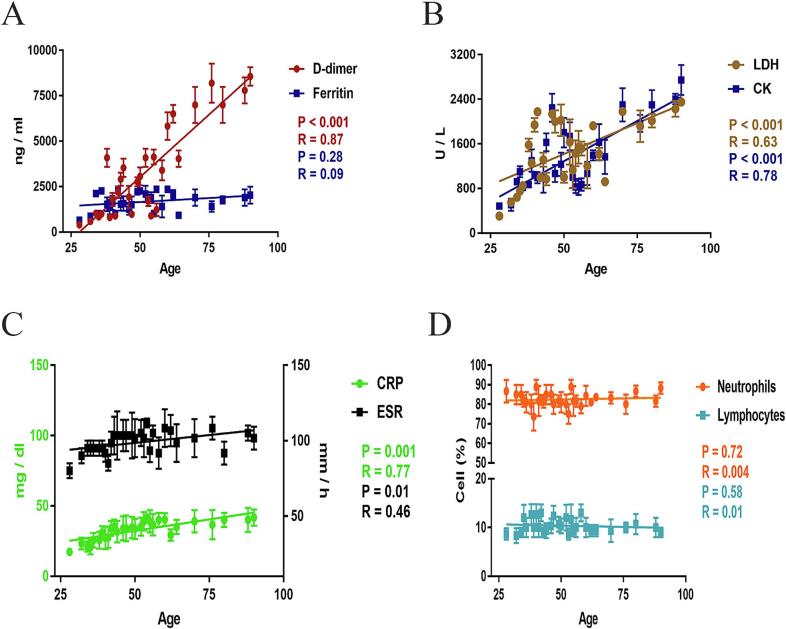
The mean age of the COVID-19 patients was 50 ± 15 years, 76.36% were male and 23.64% were female. Weight loss, sore throat, whooping cough, chest pain, and vomiting were common symptoms, and asthma, diabetes, arthritis, and hypertension were found as co-morbidities in COVID-TB. The D-dimer, lactate dehydrogenase, C-reactive protein, erythrocyte sedimentation rate, and creatine kinase levels increased 14-fold, 12.5-fold, 11-fold, 10-fold, and 7-fold respectively during COVID-TB. The patients suffered from hyperferritinemia and lymphocytopenia which increased the likelihood of death. The levels of D-dimer, lactate dehydrogenase, C-reactive protein, erythrocyte sedimentation rate, and creatinine kinase were positively correlated with patient age. The chest radiograph showed the infectious agents have consolidated opacity and peripheral dissemination in the lungs.
Tuberculosis coinfection augmented the severity of COVID-19 and the likelihood of death, and high vigilance is recommended for respiratory pathogens in COVID-19.
摘要 背景:2019年冠状病毒病大流行由一种源自中国武汉的新型单链RNA病毒引起,感染了190多个国家。严重急性呼吸综合征冠状病毒2(SARS-CoV-2)与结核病合并感染引起了严重的公共卫生问题,并使患者的预后和治疗复杂化。由于两者均为呼吸道疾病,其体征和症状可能重叠,并且可能对宿主产生协同作用,从而增加合并感染期间的死亡率。本研究报告了新型冠状病毒肺炎(COVID-19)与结核病合并感染(COVID-TB)患者的临床特征。
我们对2020年至2021年期间结核病患者的COVID-19感染情况进行了回顾性调查。通过聚合酶链反应(PCR)确诊SARS-CoV-2,并在入院当天记录COVID-TB的流行病学和临床 findings,并进行了25天的随访。
COVID-19患者的平均年龄为50±15岁,男性占76.36%,女性占23.64%。体重减轻、咽痛、百日咳、胸痛和呕吐是常见症状,在COVID-TB中发现哮喘、糖尿病、关节炎和高血压为合并症。在COVID-TB期间,D-二聚体、乳酸脱氢酶、C反应蛋白、红细胞沉降率和肌酸激酶水平分别升高了14倍、12.5倍、11倍、10倍和7倍。患者患有高铁蛋白血症和淋巴细胞减少症,这增加了死亡的可能性。D-二聚体、乳酸脱氢酶、C反应蛋白、红细胞沉降率和肌酐激酶水平与患者年龄呈正相关。胸部X线片显示病原体在肺部有实变影和外周播散。
结核病合并感染增加了COVID-19的严重程度和死亡可能性,建议对COVID-19中的呼吸道病原体保持高度警惕。