Department of Radiology, Division of Vascular and Interventional Radiology, Rutgers New Jersey Medical School, Newark, NJ, USA.
Diagn Interv Radiol. 2023 May 31;29(3):500-508. doi: 10.4274/dir.2022.22908. Epub 2023 Feb 27.
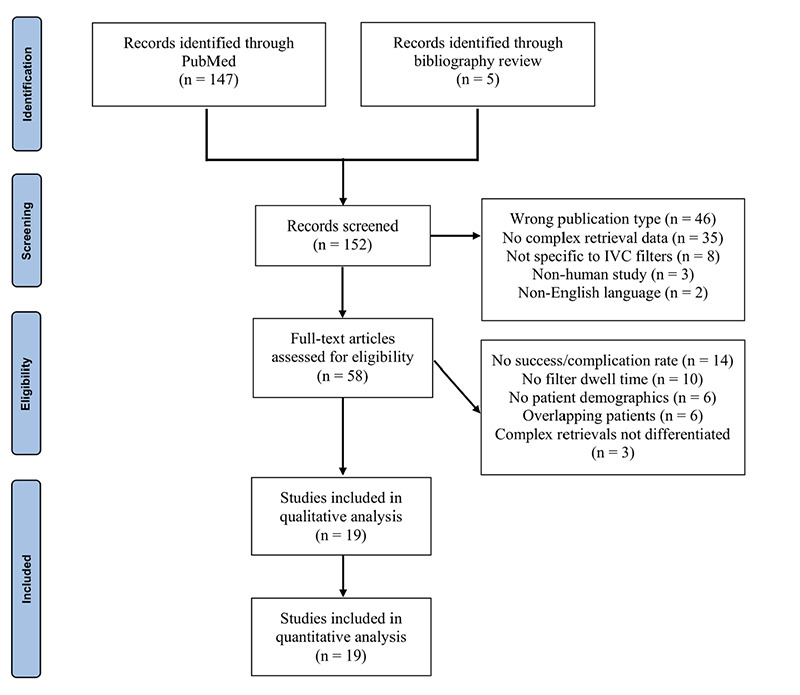
This study aimed to assess the safety of complex inferior vena cava (IVC) filter retrieval techniques through a systematic review of published literature. Using PubMed, a systematic review was conducted in line with the 2020 Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines to identify articles published through April 2020 that reported on complex IVC filter retrieval techniques in >5 patients. Case reports, review papers, and studies that did not report on primary outcomes or variables of interest were excluded. Risk of bias was assessed using a modified Newcastle-Ottawa Quality Assessment scale. Pooled success and complication rates were calculated for the overall number of complex retrieval attempts as well as for each filter type and each complex retrieval method. Sixteen fair-quality and three good-quality studies met the inclusion criteria, with 758 patients (428 female) who had undergone 770 advanced retrieval attempts. The mean age of the patients was 46.5 ± 7.1 years (range: 14.1-90), and the mean dwell time was 602.5 ± 388.6 days (range: 5-7336). Regarding filters, 92.6% (702/758) were retrievable and 7.4% (56/758) were permanent. Indications for complex retrieval included the failure of standard retrieval (89.2%; 676/758) and tilting or embedding in the caval wall (53.8%; 408/758); 92.6% (713/770) of the advanced retrieval attempts were successful. The pooled success rate was 92.0% (602/654) for retrievable filters and 96.4% (53/55) for permanent filters ( = 0.422). Only 2.8% (21/758) of patients experienced major complications, and the major complication rate was not significantly associated with filter type ( = 0.183). Advanced techniques for IVC filter retrieval appear safe for the retrieval of retrievable filters and certain permanent filters, with a low short-term major complication rate. Further studies on complex retrieval techniques used to remove permanent filters should be conducted to clarify their safety with respect to filter type.
本研究旨在通过对已发表文献的系统回顾,评估复杂下腔静脉(IVC)滤器取出技术的安全性。使用 PubMed 按照 2020 年系统评价和荟萃分析首选报告项目的指南进行了系统回顾,以确定截至 2020 年 4 月发表的超过 5 例患者报告复杂 IVC 滤器取出技术的文章。排除病例报告、综述论文以及未报告主要结局或感兴趣变量的研究。使用改良的纽卡斯尔-渥太华质量评估量表评估偏倚风险。对整体复杂取出尝试次数以及每种滤器类型和每种复杂取出方法的成功率和并发症发生率进行了汇总。符合纳入标准的 16 项质量中等和 3 项质量较高的研究共纳入 758 例患者(428 例女性),共进行了 770 次高级取出尝试。患者的平均年龄为 46.5 ± 7.1 岁(范围:14.1-90 岁),平均留置时间为 602.5 ± 388.6 天(范围:5-7336 天)。关于滤器,92.6%(702/758)可取出,7.4%(56/758)为永久性。复杂取出的指征包括标准取出失败(89.2%;676/758)和倾斜或嵌入腔静脉壁(53.8%;408/758);770 次高级取出尝试中 92.6%(713/770)成功。可取出滤器的总体取出成功率为 92.0%(602/654),永久性滤器为 96.4%(53/55)( = 0.422)。仅有 2.8%(21/758)的患者发生严重并发症,且严重并发症发生率与滤器类型无显著相关性( = 0.183)。IVC 滤器取出的高级技术对于可取出滤器和某些永久性滤器的取出似乎是安全的,短期严重并发症发生率较低。应进一步开展关于用于取出永久性滤器的复杂取出技术的研究,以明确其与滤器类型相关的安全性。