Meertens Marinda, Muntinghe-Wagenaar M Benthe, Sikkema Barend J, Lopez-Yurda Marta, Retèl Valesca P, Paats Marthe S, Ter Heine Rob, Schuuring Ed, Timens Wim, Touw Daan J, van Boven Job F M, de Langen Adrianus J, Hashemi Sayed M S, Hendriks Lizza E L, Croes Sander, van den Heuvel Michel M, Dingemans Anne-Marie C, Mathijssen Ron H J, Smit Egbert F, Huitema Alwin D R, Steeghs Neeltje, van der Wekken Anthonie J
Department of Pharmacy and Pharmacology, Netherlands Cancer Institute, Amsterdam, Netherlands.
Department of Pulmonology and Tuberculosis, University of Groningen, University Medical Center Groningen, Groningen, Netherlands.
Front Oncol. 2023 Mar 9;13:1136221. doi: 10.3389/fonc.2023.1136221. eCollection 2023.
Alectinib is first-line therapy in patients with stage IV non-small cell lung carcinoma (NSCLC) and an anaplastic lymphoma kinase (ALK) fusion. A shorter median progression-free survival (mPFS) was observed when alectinib minimum plasma concentrations during steady state (C) were below 435 ng/mL. This may suggest that patients should have an alectinib C ≥ 435 ng/mL for a more favorable outcome. This potential target could be attained by using therapeutic drug monitoring (TDM), i.e. adjusting the dose based on measured plasma trough concentrations. Hypothetically, this will increase mPFS, but this has not yet been evaluated in a randomized controlled trial (RCT). Therefore, the ADAPT ALEC trial is designed, with the primary objective to prolong mPFS in NSCLC patients treated with alectinib by using TDM.
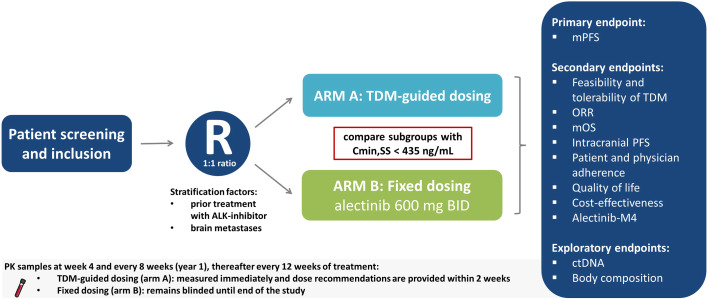
ADAPT ALEC is a multicenter, phase IV RCT, in which patients aged ≥ 18 years with advanced ALK positive (+) NSCLC eligible for alectinib in daily care are enrolled. Participants will be randomized (1:1 ratio) into intervention arm A (TDM) or B (control), stratified by brain metastases and prior ALK treatments. Starting dose in both arms is the approved flat fixed dose of alectinib 600 mg taken twice daily with food. In case of alectinib C < 435 ng/mL, arm A will receive increased doses of alectinib till C ≥ 435 ng/mL when considered tolerable. The primary outcome is mPFS, where progressive disease is defined according to RECIST v1.1 or all-cause death and assessed by CT-scans and MRI brain. Secondary endpoints are feasibility and tolerability of TDM, patient and physician adherence, overall response rate, median overall survival, intracranial PFS, quality of life, toxicity, alectinib-M4 concentrations and cost-effectiveness of TDM. Exploratory endpoints are circulating tumor DNA and body composition.
The ADAPT ALEC will show whether treatment outcomes of patients with advanced ALK+ NSCLC improve when using TDM-guided dosing of alectinib instead of fixed dosing. The results will provide high quality evidence for deciding whether TDM should be implemented as standard of care and this will have important consequences for the prescribing of alectinib.
ClinicalTrials.gov, identifier NCT05525338.
阿来替尼是晚期非小细胞肺癌(NSCLC)伴间变性淋巴瘤激酶(ALK)融合患者的一线治疗药物。当稳态时阿来替尼的最低血浆浓度(C)低于435 ng/mL时,观察到中位无进展生存期(mPFS)较短。这可能表明患者的阿来替尼C≥435 ng/mL时预后更佳。通过治疗药物监测(TDM),即根据测得的血浆谷浓度调整剂量,可能达到这一潜在目标。假设这将增加mPFS,但尚未在随机对照试验(RCT)中进行评估。因此,设计了ADAPT ALEC试验,其主要目的是通过TDM延长接受阿来替尼治疗的NSCLC患者的mPFS。
ADAPT ALEC是一项多中心IV期RCT,纳入年龄≥18岁、日常护理中符合使用阿来替尼条件的晚期ALK阳性(+)NSCLC患者。参与者将按1:1比例随机分为干预组A(TDM)或B(对照组),按脑转移和既往ALK治疗情况分层。两组的起始剂量均为已获批的阿来替尼固定剂量600 mg,每日两次,与食物同服。如果阿来替尼C<435 ng/mL,在可耐受的情况下,A组将增加阿来替尼剂量直至C≥435 ng/mL。主要结局是mPFS,其中疾病进展根据RECIST v1.1定义或全因死亡,并通过CT扫描和脑部MRI评估。次要终点是TDM的可行性和耐受性、患者和医生的依从性、总缓解率、中位总生存期、颅内PFS、生活质量、毒性、阿来替尼-M4浓度以及TDM的成本效益。探索性终点是循环肿瘤DNA和身体成分。
ADAPT ALEC将表明,对于晚期ALK+ NSCLC患者,使用TDM指导的阿来替尼给药而非固定剂量给药时,治疗结局是否会改善。结果将为决定是否应将TDM作为标准治疗提供高质量证据,这将对阿来替尼的处方产生重要影响。
ClinicalTrials.gov,标识符NCT05525338。