The University of Sydney, Sydney, NSW.
Computer Simulation and Advanced Research Technologies (CSART), Sydney, NSW.
Med J Aust. 2023 Apr 17;218(7):309-314. doi: 10.5694/mja2.51903. Epub 2023 Mar 27.
To simulate the impact on population mental health indicators of allowing people to book some Medicare-subsidised sessions with psychologists and other mental health care professionals without a referral (direct access), and of increasing the annual growth rate in specialist mental health care capacity (consultations).
System dynamics model, calibrated using historical time series data from the Australian Bureau of Statistics, HealthStats NSW, the Australian Institute of Health and Welfare, and the Australian Early Development Census. Parameter values that could not be derived from these sources were estimated by constrained optimisation.
New South Wales, 1 September 2021 - 1 September 2028.
Projected mental health-related emergency department presentations, hospitalisations following self-harm, and deaths by suicide, both overall and for people aged 15-24 years.
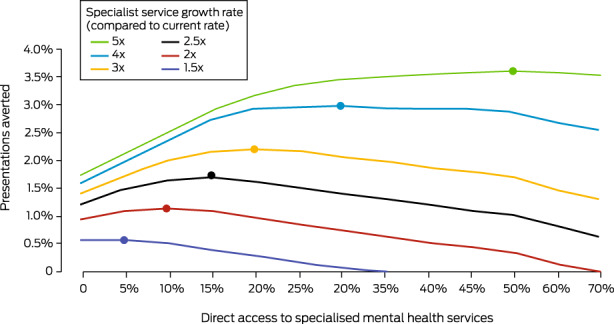
Direct access (for 10-50% of people requiring specialist mental health care) would lead to increases in the numbers of mental health-related emergency department presentations (0.33-1.68% of baseline), hospitalisations with self-harm (0.16-0.77%), and deaths by suicide (0.19-0.90%), as waiting times for consultations would increase, leading to disengagement and consequently to increases in adverse outcomes. Increasing the annual rate of growth of mental health service capacity (two- to fivefold) would reduce the frequency of all three outcomes; combining direct access to a proportion of services with increased growth in capacity achieved substantially greater gains than an increase in service capacity alone. A fivefold increase in the annual service growth rate would increase capacity by 71.6% by the end of 2028, compared with current projections; combined with direct access to 50% of mental health consultations, 26 616 emergency department presentations (3.6%), 1199 hospitalisations following self-harm (1.9%), and 158 deaths by suicide (2.1%) could be averted.
The optimal combination of increased service capacity growth (fivefold) and direct access (50% of consultations) would have double the impact over seven years of accelerated capacity growth alone. Our model highlights the risks of implementing individual reforms without knowledge of their overall system effect.
模拟允许人们在没有转介的情况下(直接就诊)预约部分医疗保险补贴的心理咨询和其他心理健康护理服务,以及增加精神卫生保健能力(咨询)年度增长率对人口心理健康指标的影响。
使用澳大利亚统计局、新南威尔士州卫生统计数据、澳大利亚健康与福利研究所和澳大利亚早期发展普查的历史时间序列数据进行校准的系统动力学模型。无法从这些来源中得出的参数值通过约束优化进行估计。
2021 年 9 月 1 日至 2028 年 9 月 1 日,新南威尔士州。
总体和 15-24 岁人群的心理健康相关急诊就诊、自残后住院和自杀死亡的预期数量。
直接就诊(10-50%需要精神卫生保健的人)将导致心理健康相关急诊就诊人数增加(基线的 0.33-1.68%)、自残后住院人数增加(0.16-0.77%)和自杀死亡人数增加(0.19-0.90%),因为咨询的等待时间会增加,导致脱诊,从而增加不良后果的发生。增加精神卫生服务能力的年度增长率(两倍到五倍)将减少所有三种结果的频率;将部分服务的直接就诊与服务能力的增长相结合,比仅增加服务能力获得更大的收益。到 2028 年底,服务年增长率增加五倍将使能力增加 71.6%;与当前预测相比,与 50%的心理健康咨询相结合,可避免 26616 次急诊就诊(3.6%)、1199 次自残后住院(1.9%)和 158 例自杀死亡(2.1%)。
增加服务能力增长(五倍)和直接就诊(50%的咨询)的最佳组合在七年的时间里将产生比仅加速能力增长两倍的影响。我们的模型强调了在不了解其整体系统效果的情况下实施单独改革的风险。