Sagami Ryota, Mizukami Kazuhiro, Okamoto Kazuhisa, Noguchi Chishio, Sato Takao, Nishikiori Hidefumi, Kawahara Yoshinari, Wada Masahiro, Otsuka Yuichiro, Fukuchi Satoshi, Takihara Hiroshi, Kuraoka Naosuke, Suzuki Keita, Murakami Kazunari
Department of Gastroenterology, Oita San-ai Medical Center, 1213 Oaza Ichi, Oita 870-1151, Japan.
Department of Gastroenterology, Faculty of Medicine, Oita University, 1-1 Idaigaoka, Hasamacho, Yufu 879-5593, Japan.
J Clin Med. 2023 Mar 20;12(6):2393. doi: 10.3390/jcm12062393.
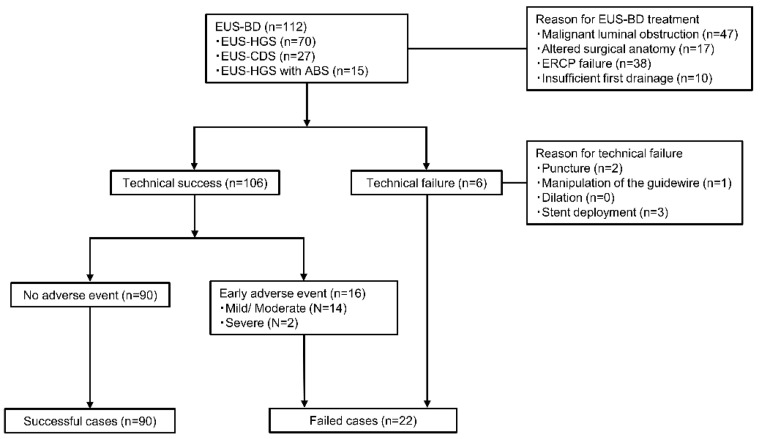
Endoscopic ultrasound-guided biliary drainage (EUS-BD) has become comparable to endoscopic retrograde cholangiopancreatography and is now considered a first-line intervention for certain biliary obstructions. Although analysis of experience-related factors may help achieve better outcomes and contribute to its wider adoption, no concrete evidence exists regarding the required operator or institutional experience levels. This study aimed to analyze experience-related factors at beginner multicenters. Patients who underwent EUS-BD using self-expandable metal stents and/or dedicated plastic stents during the study period (up to the first 25 cases since introducing the technique) were retrospectively enrolled from seven beginner institutions and operators. Overall, 90 successful (technical success without early adverse events) and 22 failed (technical failure and/or early adverse events) cases were compared. EUS-BD-related procedures conducted at the time of applicable EUS-BD by each institution/operator were evaluated. The number of institution-conducted EUS-BD procedures (≥7) and operator-conducted EUS screenings (≥436), EUS-guided fine-needle aspirations (FNA) (≥93), and EUS-guided drainages (≥13) significantly influenced improved EUS-BD outcomes ( = 0.022, odds ratio [OR], 3.0; = 0.022, OR, 3.0; = 0.022, OR, 3.0; and = 0.028, OR, 2.9, respectively). Our threshold values, which significantly divided successful and failed cases, were assessed using receiver operating characteristic curve analysis and may provide useful approximate indications for successful EUS-BD.
内镜超声引导下胆管引流术(EUS - BD)已变得与内镜逆行胰胆管造影术相当,目前被视为某些胆管梗阻的一线干预措施。尽管分析与经验相关的因素可能有助于取得更好的结果并促进其更广泛的应用,但关于所需的操作者或机构经验水平尚无具体证据。本研究旨在分析初学者多中心的经验相关因素。在研究期间(自引入该技术起至首批25例病例),使用自膨式金属支架和/或专用塑料支架接受EUS - BD的患者从7个初学者机构和操作者中进行回顾性纳入。总体而言,对90例成功(无早期不良事件的技术成功)和22例失败(技术失败和/或早期不良事件)病例进行了比较。对每个机构/操作者在适用的EUS - BD时进行的与EUS - BD相关的操作进行了评估。机构进行的EUS - BD操作数量(≥7)以及操作者进行的EUS筛查(≥436)、EUS引导下细针穿刺抽吸术(FNA)(≥93)和EUS引导下引流术(≥13)对改善EUS - BD结果有显著影响(分别为 = 0.022,优势比[OR],3.0; = 0.022,OR,3.0; = 0.022,OR,3.0;以及 = 0.028,OR,2.9)。我们使用受试者工作特征曲线分析评估了显著区分成功和失败病例的阈值,这些阈值可能为成功的EUS - BD提供有用的近似指标。