Sanfilippo Filippo, La Via Luigi, Dezio Veronica, Santonocito Cristina, Amelio Paolo, Genoese Giulio, Astuto Marinella, Noto Alberto
Department of Anaesthesia and Intensive Care, A.O.U. Policlinico-San Marco, site "Policlinico G. Rodolico", Via S. Sofia N 78, 95123, Catania, Italy.
School of Anaesthesia and Intensive Care, University Hospital "G. Rodolico", University of Catania, 95123, Catania, Italy.
Intensive Care Med Exp. 2023 Apr 3;11(1):15. doi: 10.1186/s40635-023-00505-7.
Assessment of the inferior vena cava (IVC) respiratory variation may be clinically useful for the estimation of fluid-responsiveness and venous congestion; however, imaging from subcostal (SC, sagittal) region is not always feasible. It is unclear if coronal trans-hepatic (TH) IVC imaging provides interchangeable results. The use of artificial intelligence (AI) with automated border tracking may be helpful as part of point-of-care ultrasound but it needs validation.
Prospective observational study conducted in spontaneously breathing healthy volunteers with assessment of IVC collapsibility (IVCc) in SC and TH imaging, with measures taken in M-mode or with AI software. We calculated mean bias and limits of agreement (LoA), and the intra-class correlation (ICC) coefficient with their 95% confidence intervals.
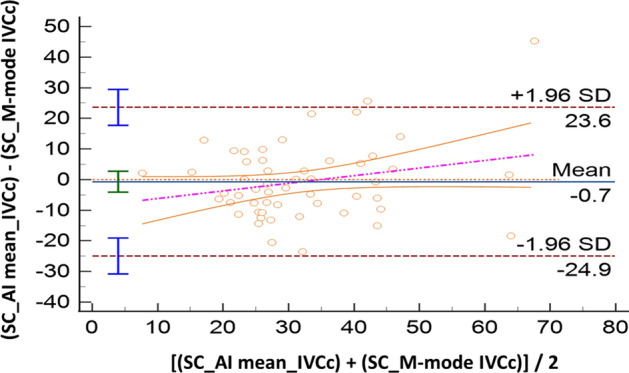
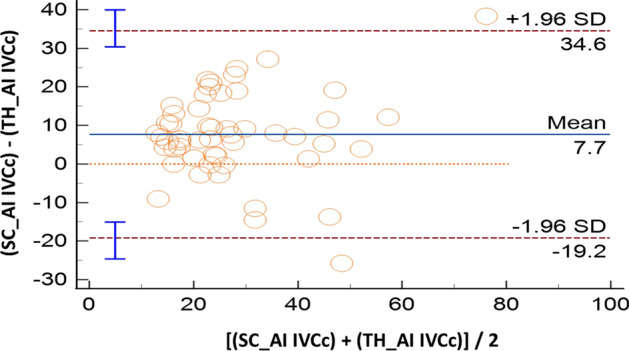
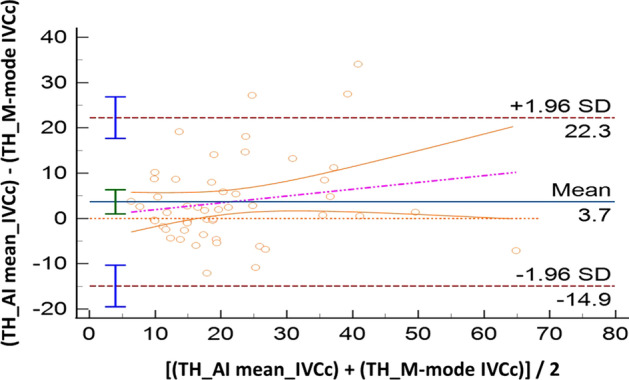
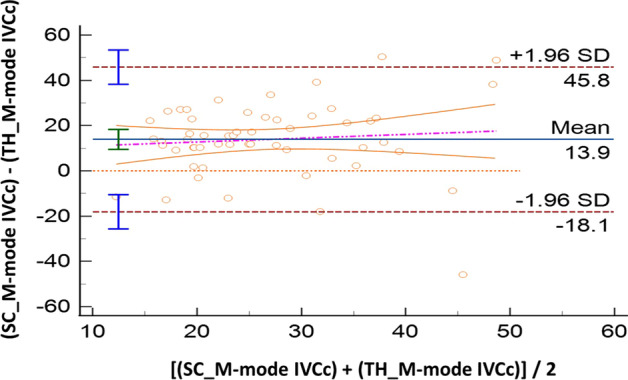
Sixty volunteers were included; IVC was not visualized in five of them (n = 2, both SC and TH windows, 3.3%; n = 3 in TH approach, 5%). Compared with M-mode, AI showed good accuracy both for SC (IVCc: bias - 0.7%, LoA [- 24.9; 23.6]) and TH approach (IVCc: bias 3.7%, LoA [- 14.9; 22.3]). The ICC coefficients showed moderate reliability: 0.57 [0.36; 0.73] in SC, and 0.72 [0.55; 0.83] in TH. Comparing anatomical sites (SC vs TH), results produced by M-mode were not interchangeable (IVCc: bias 13.9%, LoA [- 18.1; 45.8]). When this evaluation was performed with AI, such difference became smaller: IVCc bias 7.7%, LoA [- 19.2; 34.6]. The correlation between SC and TH assessments was poor for M-mode (ICC = 0.08 [- 0.18; 0.34]) while moderate for AI (ICC = 0.69 [0.52; 0.81]).
The use of AI shows good accuracy when compared with the traditional M-mode IVC assessment, both for SC and TH imaging. Although AI reduces differences between sagittal and coronal IVC measurements, results from these sites are not interchangeable.
评估下腔静脉(IVC)呼吸变异对于估计液体反应性和静脉充血可能具有临床意义;然而,从肋下(SC,矢状面)区域进行成像并不总是可行的。目前尚不清楚冠状面经肝(TH)IVC成像是否能提供可互换的结果。在床旁超声检查中使用具有自动边界跟踪功能的人工智能(AI)可能会有所帮助,但需要进行验证。
对自主呼吸的健康志愿者进行前瞻性观察研究,评估SC和TH成像中的IVC可塌陷性(IVCc),采用M型测量或使用AI软件进行测量。我们计算了平均偏差和一致性界限(LoA),以及组内相关系数(ICC)及其95%置信区间。
纳入60名志愿者;其中5人未观察到IVC(n = 2,SC和TH窗口均未观察到,3.3%;n = 3在TH方法中未观察到,5%)。与M型相比,AI在SC(IVCc:偏差 - 0.7%,LoA [- 24.9;23.6])和TH方法(IVCc:偏差3.7%,LoA [- 14.9;22.3])中均显示出良好的准确性。ICC系数显示出中等可靠性:SC为0.57 [0.36;0.73],TH为0.72 [0.55;0.83]。比较解剖部位(SC与TH),M型产生的结果不可互换(IVCc:偏差13.9%,LoA [- 18.1;45.8])。当使用AI进行此评估时,这种差异变小:IVCc偏差7.7%,LoA [- 19.2;34.6]。M型的SC和TH评估之间的相关性较差(ICC = 0.08 [- 0.18;0.34]),而AI的相关性中等(ICC = 0.69 [0.52;0.81])。
与传统的M型IVC评估相比,AI在SC和TH成像中均显示出良好的准确性。虽然AI减少了矢状面和冠状面IVC测量之间的差异,但这些部位的结果不可互换。