Department of Biliary-Pancreatic Surgery, Affiliated Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei Province, China.
Int J Surg. 2023 Apr 1;109(4):660-669. doi: 10.1097/JS9.0000000000000180.
It remains uncertain how surgeons can safely pass the learning curve of laparoscopic pancreatoduodenectomy (LPD) without potentially harming patients. We aimed to develop a difficulty scoring system (DSS) to select an appropriate patient for surgeons.
A total of 773 elective pancreatoduodenectomy surgeries between July 2014 and December 2019, including 346 LPD and 427 open pancreatoduodenectomy cases, were included. A 10-level DSS for LPD was developed, and an additional 77 consecutive LPD surgeries which could provide information of the learning stage I of LPD externally validated its performance between December 2019 and December 2021.
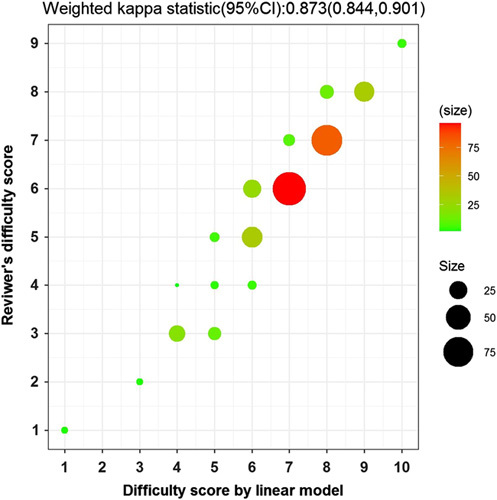
The incidences of postoperative complications (Clavien-Dindo≥III) gradually decreased from the learning curve stage I-III (20.00, 10.94, 5.79%, P =0.008, respectively). The DSS consisted of the following independent risk factors: (1) tumor location, (2) vascular resection and reconstruction, (3) learning curve stage, (4) prognostic nutritional index, (5) tumor size, and (6) benign or malignant tumor. The weighted Cohen's κ statistic of concordance between the reviewer's and calculated difficulty score index was 0.873. The C -statistics of DSS for postoperative complication (Clavien-Dindo≥III) were 0.818 in the learning curve stage I. The patients with DSS<5 had lower postoperative complications (Clavien-Dindo≥III) than those with DSS≥5 (4.35-41.18%, P =0.004) in the training cohort and had a lower postoperative pancreatic fistula (19.23-57.14%, P =0.0352), delayed gastric emptying (19.23-71.43%, P =0.001), and bile leakage rate (0.00-21.43%, P =0.0368) in validation cohort in the learning curve stage I.
We developed and validated a difficulty score model for patient selection, which could facilitate the stepwise adoption of LPD for surgeons at different stages of the learning curve.
目前仍不清楚外科医生如何在不伤害患者的情况下安全地跨越腹腔镜胰十二指肠切除术(LPD)的学习曲线。我们旨在开发一种困难评分系统(DSS),以便为外科医生选择合适的患者。
纳入 2014 年 7 月至 2019 年 12 月期间的 773 例择期胰十二指肠切除术,其中 346 例为 LPD,427 例为开腹胰十二指肠切除术。建立了 LPD 的 10 级 DSS,并在 2019 年 12 月至 2021 年 12 月期间连续进行了 77 例 LPD 手术,以提供 LPD 学习阶段 I 的信息来外部验证其性能。
术后并发症(Clavien-Dindo≥III)的发生率从学习曲线阶段 I-III 逐渐降低(20.00、10.94、5.79%,P=0.008)。DSS 包括以下独立危险因素:(1)肿瘤位置,(2)血管切除和重建,(3)学习曲线阶段,(4)预后营养指数,(5)肿瘤大小,(6)良性或恶性肿瘤。审核者和计算出的难度评分指数之间的加权 Cohen's κ 一致性统计量为 0.873。DSS 对术后并发症(Clavien-Dindo≥III)的 C 统计量在学习曲线阶段 I 为 0.818。在训练队列中,DSS<5 的患者术后并发症(Clavien-Dindo≥III)发生率低于 DSS≥5 的患者(4.35-41.18%,P=0.004),在学习曲线阶段 I,术后胰瘘(19.23-57.14%,P=0.0352)、胃排空延迟(19.23-71.43%,P=0.001)和胆漏发生率(0.00-21.43%,P=0.0368)均较低。在验证队列中,在学习曲线阶段 I,DSS<5 的患者术后并发症(Clavien-Dindo≥III)发生率低于 DSS≥5 的患者(4.35-41.18%,P=0.004),术后胰瘘(19.23-57.14%,P=0.0352)、胃排空延迟(19.23-71.43%,P=0.001)和胆漏发生率(0.00-21.43%,P=0.0368)均较低。
我们开发并验证了一种患者选择的困难评分模型,该模型可以帮助外科医生在学习曲线的不同阶段逐步采用 LPD。