Department of Medicine, Division of Infectious Diseases, Duke University Medical Center, Durham, North Carolina.
Duke Clinical Research Institute, Durham, North Carolina.
JAMA Netw Open. 2023 Apr 3;6(4):e238516. doi: 10.1001/jamanetworkopen.2023.8516.
Limited effective therapeutics are available to hospitalized patients with COVID-19. Clinical trials and observational studies have shown varying effects of systemic corticosteroids, including dexamethasone, in hospitalized patients with COVID-19, with limited descriptions of important patient subgroups.
To examine the clinical use of dexamethasone for hospitalized patients with COVID-19 respiratory illness and to explore the heterogeneity of treatment outcomes across different subgroups.
DESIGN, SETTING, AND PARTICIPANTS: This is a retrospective, propensity score-weighted cohort study of adult patients hospitalized for at least 48 hours for COVID-19 respiratory illness between July 1, 2020, and October 31, 2021, at a large health care network of 156 hospitals across the US. Data analysis was performed from March 2022 to February 2023.
Systemic dexamethasone administered within 48 hours of either admission or escalation in oxygen support.
All-cause in-hospital mortality or discharge to hospice.
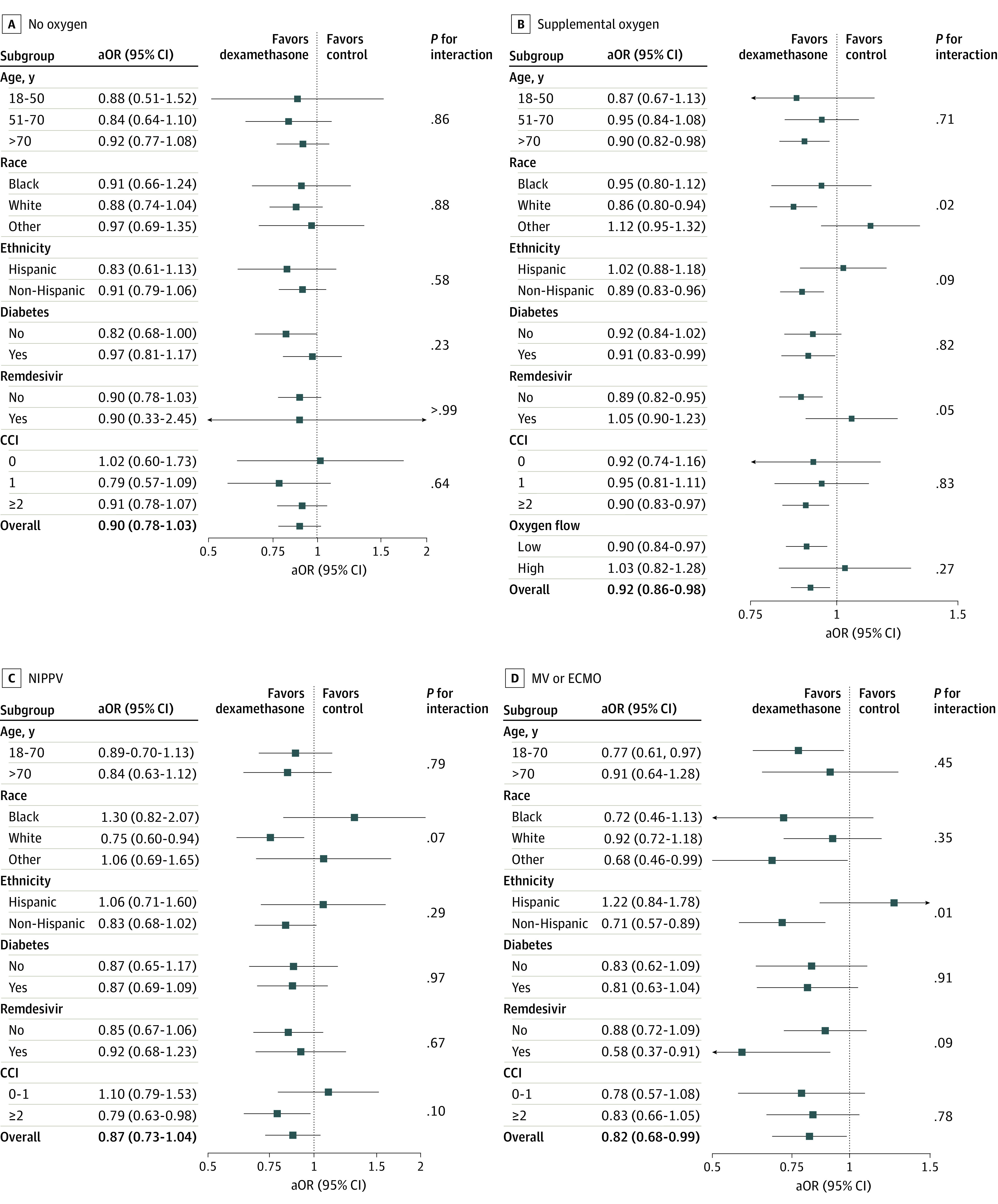
A total of 80 699 patients who met the eligibility criteria were identified (median [IQR] age, 64 [52-76] years; 37 606 women [46.6%]); 13 230 patients (16.4%) identified as Black, 49 222 (60.9%) as White, 18 247 (22.6%) as other race, and 20 340 (25.2%) as Hispanic ethnicity. Of these patients, 13 040 (16.2%) did not require supplemental oxygen within 48 hours of admission, 56 368 (69.8%) required supplemental oxygen, 7618 (9.4%) required noninvasive positive pressure ventilation (NIPPV), and 3673 (4.6%) required mechanical ventilation (MV) and/or extracorporeal membrane oxygenation (ECMO). After adjustment by propensity score overlap weighting, early use of dexamethasone was associated with reduction in a composite outcome of in-hospital mortality or discharge to hospice for patients receiving supplemental oxygen (aOR, 0.92; 95% CI, 0.86-0.98) and MV and/or ECMO (aOR, 0.82; 95% CI, 0.68-0.99). In contrast, all-cause inpatient mortality or discharge to hospice was not lower for patients who received dexamethasone in the no supplemental oxygen group (aOR, 0.90; 95% CI, 0.78-1.03) and in the NIPPV group (aOR, 0.87; 95% CI, 0.73-1.04). Importantly, patients with more comorbidities had greater benefit from dexamethasone use.
In this national multicenter cohort study of inpatients with COVID-19, early administration of dexamethasone was associated with significantly reduced odds of mortality or discharge to hospice in those requiring supplemental oxygen or MV and/or ECMO but not in those requiring no supplemental oxygen or NIPPV. These results support the continued use of systemic dexamethasone in patients hospitalized with COVID-19.
目前针对 COVID-19 住院患者的有效治疗方法有限。临床试验和观察性研究表明,全身性皮质类固醇(包括地塞米松)在 COVID-19 住院患者中的作用存在差异,但对重要的亚组患者描述有限。
研究地塞米松在 COVID-19 呼吸疾病住院患者中的临床应用,并探索不同亚组患者治疗结局的异质性。
设计、设置和参与者:这是一项回顾性、倾向评分加权队列研究,纳入了 2020 年 7 月 1 日至 2021 年 10 月 31 日期间美国 156 家医院的大型医疗保健网络中至少住院 48 小时的 COVID-19 呼吸疾病成年患者。数据分析于 2022 年 3 月至 2023 年 2 月进行。
入院后 48 小时内或在氧支持升级后给予全身性地塞米松。
全因住院死亡率或出院至临终关怀。
共确定了符合入选标准的 80699 名患者(中位数[IQR]年龄,64[52-76]岁;37606 名女性[46.6%]);13230 名患者(16.4%)被认定为黑人,49222 名(60.9%)为白人,18247 名(22.6%)为其他种族,20340 名(25.2%)为西班牙裔。这些患者中,13040 名(16.2%)在入院后 48 小时内不需要补充氧气,56368 名(69.8%)需要补充氧气,7618 名(9.4%)需要无创正压通气(NIPPV),3673 名(4.6%)需要机械通气(MV)和/或体外膜氧合(ECMO)。在通过倾向评分重叠加权调整后,早期使用地塞米松与接受补充氧气的患者住院死亡率或出院至临终关怀的复合结局降低相关(比值比,0.92;95%置信区间,0.86-0.98)和 MV 和/或 ECMO(比值比,0.82;95%置信区间,0.68-0.99)。相比之下,接受地塞米松的患者在不接受补充氧气组(比值比,0.90;95%置信区间,0.78-1.03)和 NIPPV 组(比值比,0.87;95%置信区间,0.73-1.04)的全因住院死亡率或出院至临终关怀率并没有降低。重要的是,合并症较多的患者从地塞米松治疗中获益更大。
在这项针对 COVID-19 住院患者的全国多中心队列研究中,早期给予地塞米松与需要补充氧气或 MV 和/或 ECMO 的患者的死亡率或出院至临终关怀的几率显著降低相关,但与不需要补充氧气或 NIPPV 的患者无关。这些结果支持在 COVID-19 住院患者中继续使用全身性地塞米松。