Institute for Public Health Genetics, University of Washington, Seattle, WA, USA.
Department of Laboratory Medicine and Pathology, University of Washington, Rm NW120, Box 357110 1959 NE Pacific Street, WA, 98195, Seattle, USA.
Genome Med. 2023 Apr 18;15(1):26. doi: 10.1186/s13073-023-01174-7.
Population screening for genetic risk of adult-onset preventable conditions has been proposed as an attractive public health intervention. Screening unselected individuals can identify many individuals who will not be identified through current genetic testing guidelines.
We sought to evaluate enrollment in and diagnostic yield of population genetic screening in a resource-limited setting among a diverse population. We developed a low-cost, short-read next-generation sequencing panel of 25 genes that had 98.4% sensitivity and 99.98% specificity compared to diagnostic panels. We used email invitations to recruit a diverse cohort of patients in the University of Washington Medical Center system unselected for personal or family history of hereditary disease. Participants were sent a saliva collection kit in the mail with instructions on kit use and return. Results were returned using a secure online portal. Enrollment and diagnostic yield were assessed overall and across race and ethnicity groups.
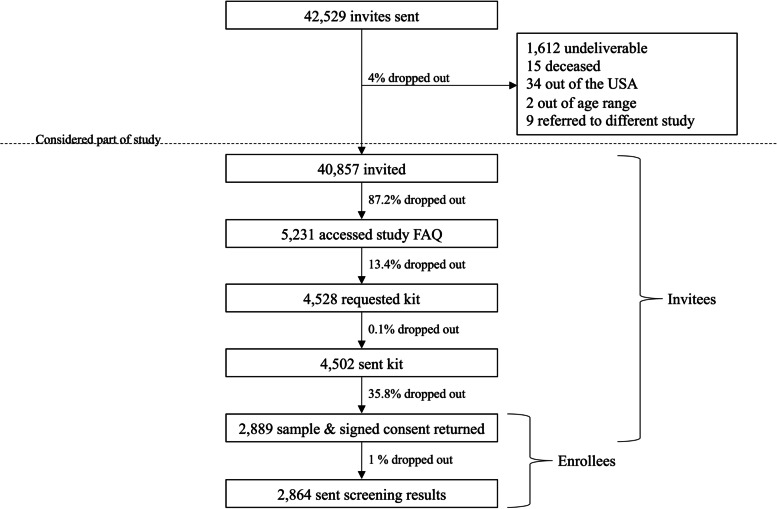
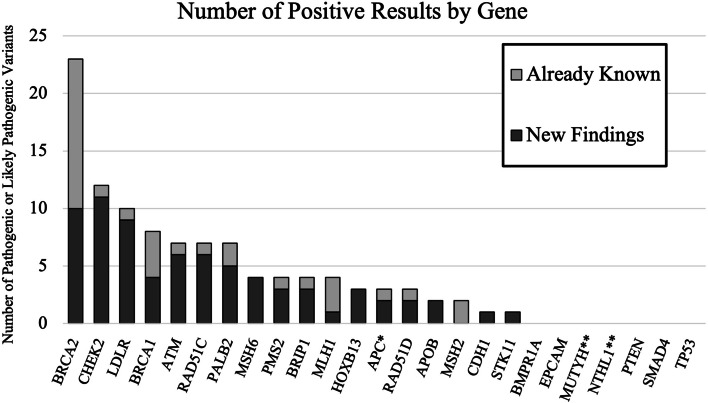
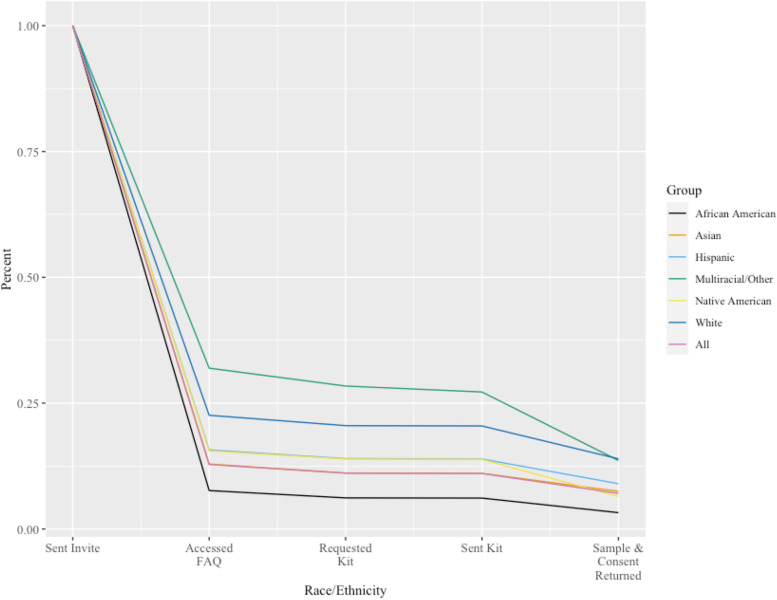
Overall, 40,857 people were invited and 2889 (7.1%) enrolled. Enrollment varied across race and ethnicity groups, with the lowest enrollment among African American individuals (3.3%) and the highest among Multiracial or Other Race individuals (13.0%). Of 2864 enrollees who received screening results, 106 actionable variants were identified in 103 individuals (3.6%). Of those who screened positive, 30.1% already knew about their results from prior genetic testing. The diagnostic yield was 74 new, actionable genetic findings (2.6%). The addition of more recently identified cancer risk genes increased the diagnostic yield of screening.
Population screening can identify additional individuals that could benefit from prevention, but challenges in recruitment and sample collection will reduce actual enrollment and yield. These challenges should not be overlooked in intervention planning or in cost and benefit analysis.
人群筛查成年发病可预防疾病的遗传风险,被认为是一种有吸引力的公共卫生干预措施。对未选择个体进行筛查,可以发现许多通过当前遗传检测指南无法识别的个体。
我们试图在资源有限的环境中,在一个多样化的人群中评估人群遗传筛查的参与度和诊断收益。我们开发了一种低成本、短读长的下一代测序panel,其中包含 25 个基因,与诊断panel 相比,其敏感性为 98.4%,特异性为 99.98%。我们使用电子邮件邀请在华盛顿大学医学中心系统中未选择有遗传性疾病个人或家族史的患者加入,以招募多样化的队列。参与者会通过邮件收到唾液采集套件,并附有套件使用和返回说明。结果通过安全的在线门户返回。评估了总体以及不同种族和族裔群体的参与度和诊断收益。
共有 40857 人受邀,2889 人(7.1%)参与。参与度因种族和族裔群体而异,非洲裔美国人(3.3%)的参与度最低,多种族或其他种族(13.0%)的参与度最高。在 2864 名接受筛查结果的参与者中,103 名参与者(3.6%)发现了 106 个可操作的变异。在筛查阳性的人中,30.1%已经从之前的遗传检测中了解到自己的结果。诊断收益为 74 个新的、可操作的遗传发现(2.6%)。增加最近发现的癌症风险基因,提高了筛查的诊断收益。
人群筛查可以发现更多可能受益于预防的个体,但在招募和样本采集方面的挑战将降低实际参与度和收益。在干预计划或成本效益分析中,不应忽视这些挑战。