University of Gothenburg, Sahlgrenska Academy, Institute of Clinical Sciences, Gothenburg, Sweden.
Department of Research and Development, NU Hospital Group, Trollhättan, Sweden.
Br J Surg. 2023 May 16;110(6):710-716. doi: 10.1093/bjs/znad081.
Acute high-risk abdominal surgery is common, as are the attendant risks of organ failure, need for intensive care, mortality, or long hospital stay. This study assessed the implementation of standardized management.
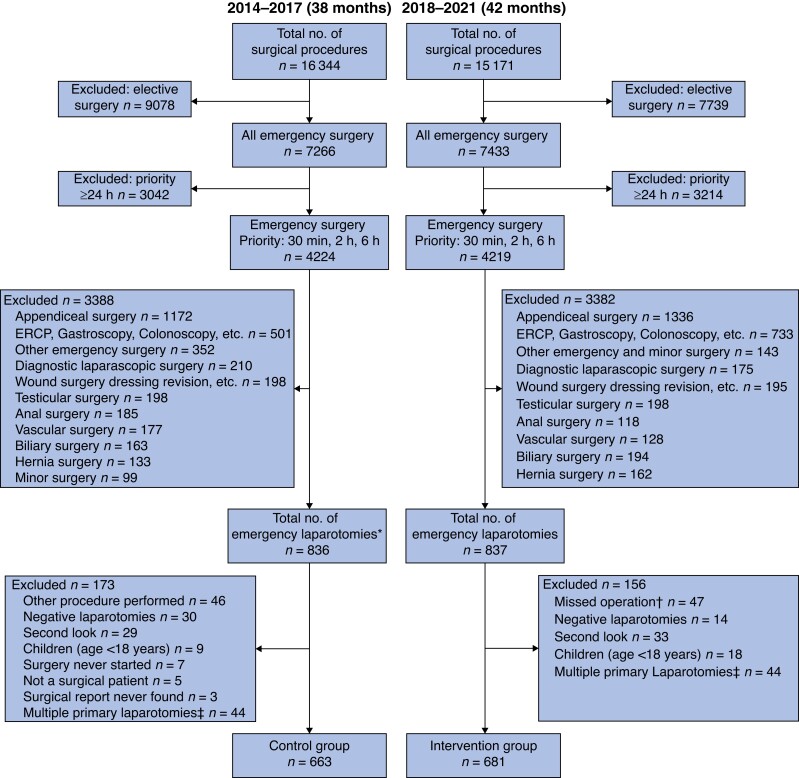
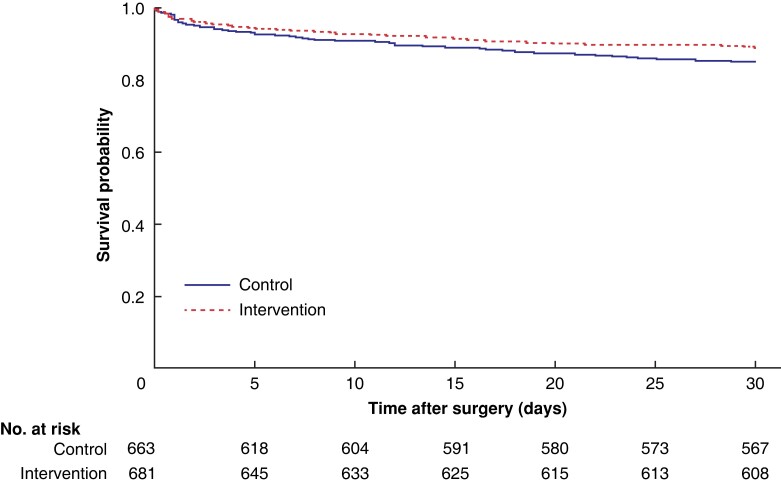
A prospective study of all adults undergoing emergency laparotomy over an interval of 42 months (2018-2021) was undertaken; outcomes were compared with those of a retrospective control group. A new standardized clinical protocol was activated for all patients including: prompt bedside physical assessment by the surgeon and anaesthetist, interprofessional communication regarding location of resuscitation, elimination of unnecessary factors that might delay surgery, improved operating theatre competence, regular epidural, enhanced recovery care, and frequent early warning scores. The primary endpoint was 30-day mortality. Secondary endpoints were duration of hospital stay, need for intensive care, and surgical complications.
A total of 1344 patients were included, 663 in the control group and 681 in the intervention group. The use of antibiotics increased (81.4 versus 94.7 per cent), and the time from the decision to operate to the start of surgery was reduced (3.80 versus 3.22 h) with use of the new protocol. Fewer anastomoses were performed (22.5 versus 16.8 per cent). The 30-day mortality rate was 14.5 per cent in the historical control group and 10.7 per cent in the intervention group (P = 0.045). The mean duration of hospital (11.9 versus 10.2 days; P = 0.007) and ICU (5.40 versus 3.12 days; P = 0.007) stays was also reduced. The rate of serious surgical complications (grade IIIb-V) was lower (37.6 versus 27.3 per cent; P = <0.001).
Standardized management protocols improved outcomes after emergency laparotomy.
急性高危腹部手术很常见,随之而来的是器官衰竭、需要重症监护、死亡率或住院时间延长的风险。本研究评估了标准化管理的实施情况。
对 42 个月(2018-2021 年)期间所有接受紧急剖腹手术的成年人进行前瞻性研究;将结果与回顾性对照组进行比较。为所有患者启动了新的标准化临床方案,包括:外科医生和麻醉师进行床边快速体格检查、多学科间就复苏地点进行沟通、消除可能延误手术的不必要因素、提高手术室能力、定期硬膜外镇痛、强化康复护理以及频繁的早期预警评分。主要终点为 30 天死亡率。次要终点为住院时间、需要重症监护和手术并发症。
共纳入 1344 例患者,其中对照组 663 例,干预组 681 例。新方案的使用增加了抗生素的使用(81.4%对 94.7%),手术决策到手术开始的时间缩短(3.80 小时对 3.22 小时)。吻合术减少(22.5%对 16.8%)。历史对照组 30 天死亡率为 14.5%,干预组为 10.7%(P=0.045)。住院(11.9 天对 10.2 天;P=0.007)和 ICU(5.40 天对 3.12 天;P=0.007)的平均停留时间也缩短。严重手术并发症(IIIb-V 级)的发生率较低(37.6%对 27.3%;P<0.001)。
标准化管理方案改善了紧急剖腹手术后的结果。