International Health, Johns Hopkins Bloomberg School of Public Health, 615 North Wolfe Street, Baltimore, MD 21205, USA.
Health Programme, UNICEF New York, 3 UN Plaza, New York, NY 10017, USA.
Health Policy Plan. 2023 May 17;38(5):631-647. doi: 10.1093/heapol/czad021.
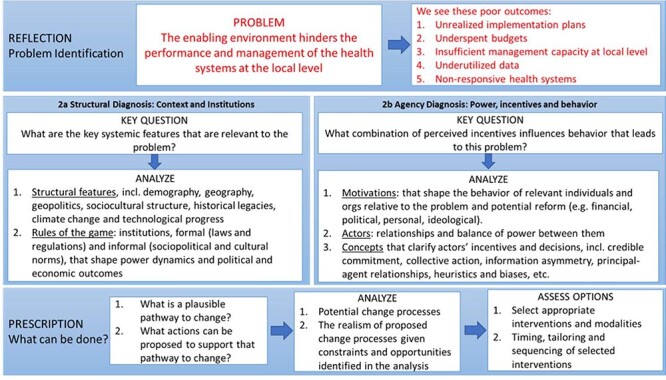
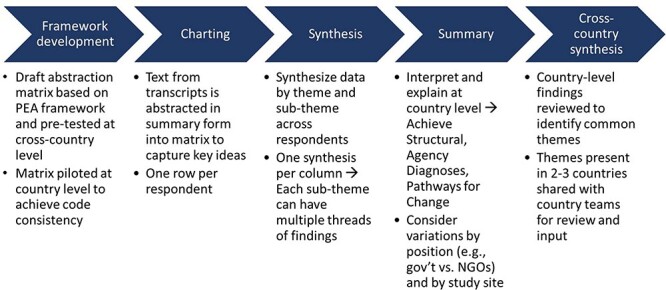
The need to bolster primary health care (PHC) to achieve the Sustainable Development Goal (SDG) targets for health is well recognized. In Eastern and Southern Africa, where governments have progressively decentralized health decision-making, health management is critical to PHC performance. While investments in health management capacity are important, so is improving the environment in which managers operate. Governance arrangements, management systems and power dynamics of actors can have a significant influence on health managers' ability to improve PHC access and quality. We conducted a problem-driven political economy analysis (PEA) in Kenya, Malawi and Uganda to explore local decision-making environments and how they affect management and governance practices for health. This PEA used document review and key informant interviews (N = 112) with government actors, development partners and civil societies in three districts or counties in each country (N = 9). We found that while decentralization should improve PHC by supporting better decisions in line with local priorities from community input, it has been accompanied by thick bureaucracy, path-dependent and underfunded budgets that result in trade-offs and unfulfilled plans, management support systems that are less aligned to local priorities, weak accountability between local government and development partners, uneven community engagement and insufficient public administration capacity to negotiate these challenges. Emergent findings suggest that coronavirus disease 2019 (COVID-19) not only resulted in greater pressures on health teams and budgets but also improved relations with central government related to better communication and flexible funding, offering some lessons. Without addressing the disconnection between the vision for decentralization and the reality of health managers mired in unhelpful processes and politics, delivering on PHC and universal health coverage goals and the SDG agenda will remain out of reach.
加强初级卫生保健(PHC)以实现卫生方面的可持续发展目标(SDG)的需求已得到充分认识。在东非和南非,政府已逐步将卫生决策权下放,因此卫生管理对于 PHC 的绩效至关重要。虽然对卫生管理能力的投资很重要,但改善管理人员的运作环境也很重要。治理安排、管理系统和行为者的权力动态对卫生管理人员改善 PHC 可及性和质量的能力具有重大影响。我们在肯尼亚、马拉维和乌干达进行了以问题为导向的政治经济分析(PEA),以探讨当地的决策环境以及这些环境如何影响卫生管理和治理实践。该 PEA 使用了文件审查和关键知情者访谈(N=112),受访者包括来自三个国家的每个国家的三个地区或县的政府行为者、发展伙伴和民间社会(N=9)。我们发现,虽然权力下放应该通过支持更好地根据社区投入制定符合当地优先事项的决策来改善 PHC,但权力下放也伴随着官僚主义浓厚、路径依赖和资金不足的预算,导致权衡取舍和计划无法兑现、管理支持系统与当地优先事项的一致性较差、地方政府与发展伙伴之间问责制薄弱、社区参与程度不均以及公共行政能力不足以应对这些挑战。新出现的发现表明,2019 冠状病毒病(COVID-19)不仅给卫生团队和预算带来了更大的压力,还改善了与中央政府的关系,这与更好的沟通和灵活的资金有关,从中吸取了一些经验教训。如果不解决权力下放的愿景与陷入无益流程和政治的卫生管理人员之间的脱节问题,实现 PHC 和全民健康覆盖目标以及可持续发展目标议程将仍然遥不可及。