Medicine, University of Calgary Cumming School of Medicine, Calgary, Alberta, Canada
Department of Electrical Engineering and Computer Science, Massachusetts Institute of Technology, Cambridge, Massachusetts, USA.
Ann Rheum Dis. 2023 Jul;82(7):927-936. doi: 10.1136/ard-2022-223808. Epub 2023 Apr 21.
A novel longitudinal clustering technique was applied to comprehensive autoantibody data from a large, well-characterised, multinational inception systemic lupus erythematosus (SLE) cohort to determine profiles predictive of clinical outcomes.
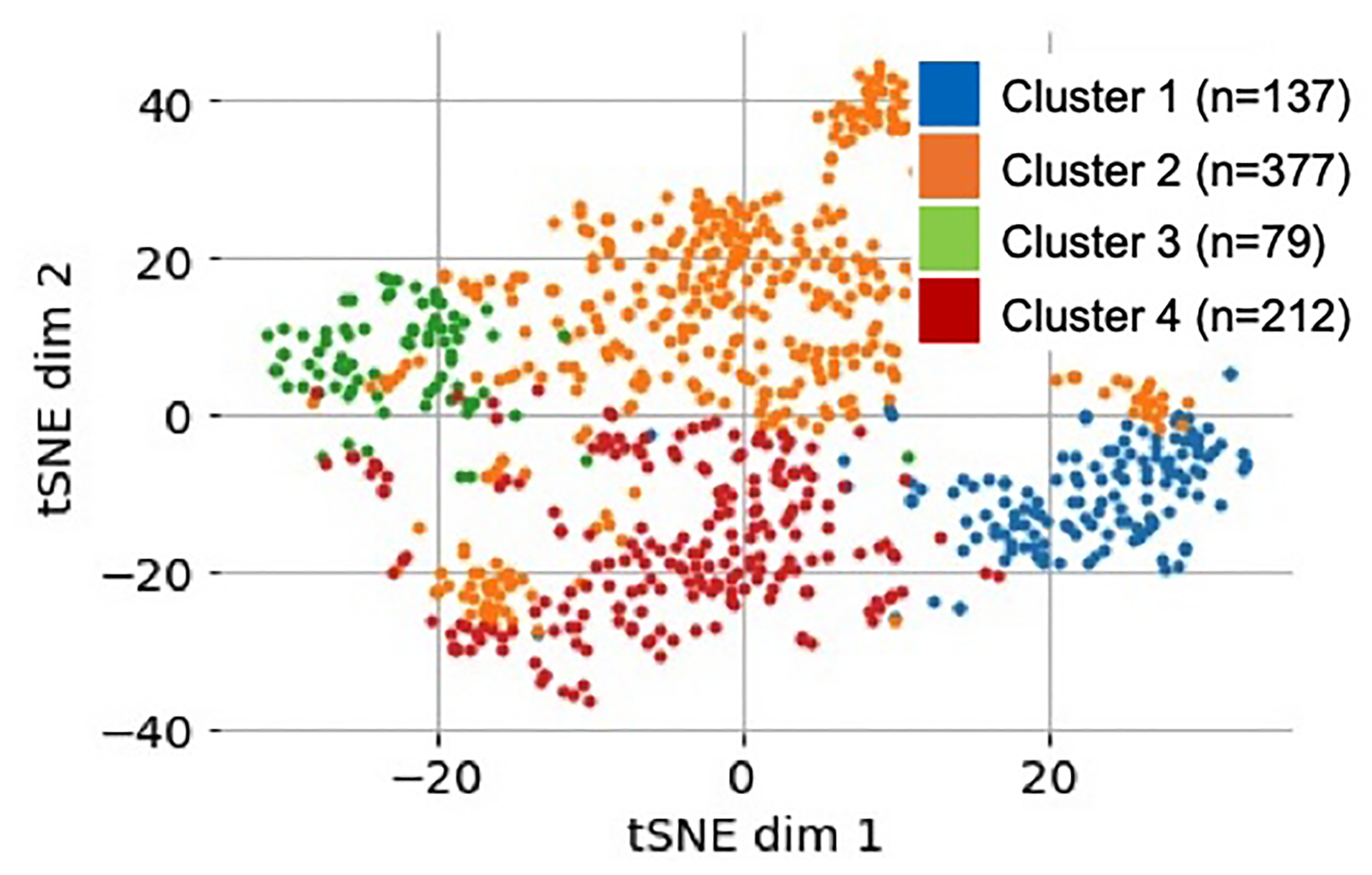
Demographic, clinical and serological data from 805 patients with SLE obtained within 15 months of diagnosis and at 3-year and 5-year follow-up were included. For each visit, sera were assessed for 29 antinuclear antibodies (ANA) immunofluorescence patterns and 20 autoantibodies. K-means clustering on principal component analysis-transformed longitudinal autoantibody profiles identified discrete phenotypic clusters. One-way analysis of variance compared cluster enrolment demographics and clinical outcomes at 10-year follow-up. Cox proportional hazards model estimated the HR for survival adjusting for age of disease onset.
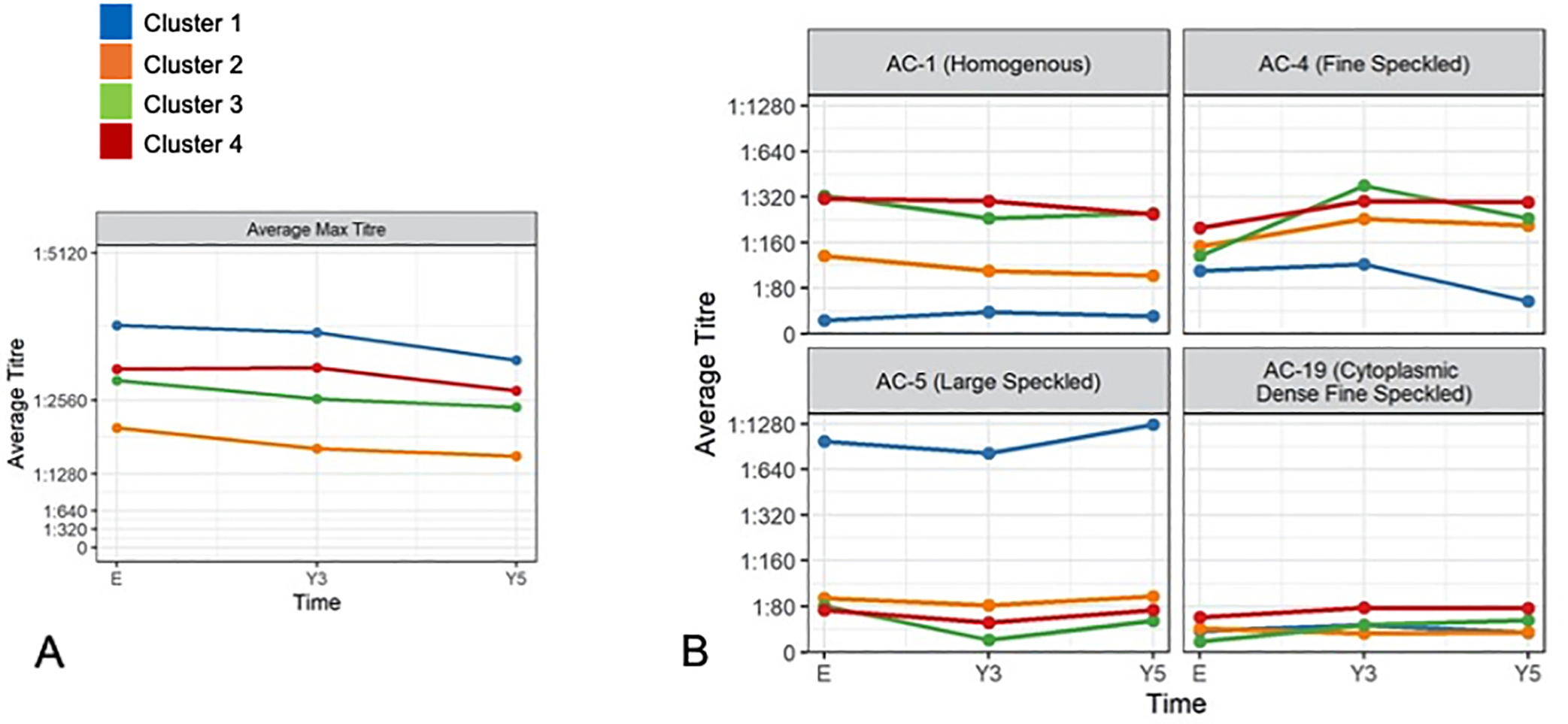
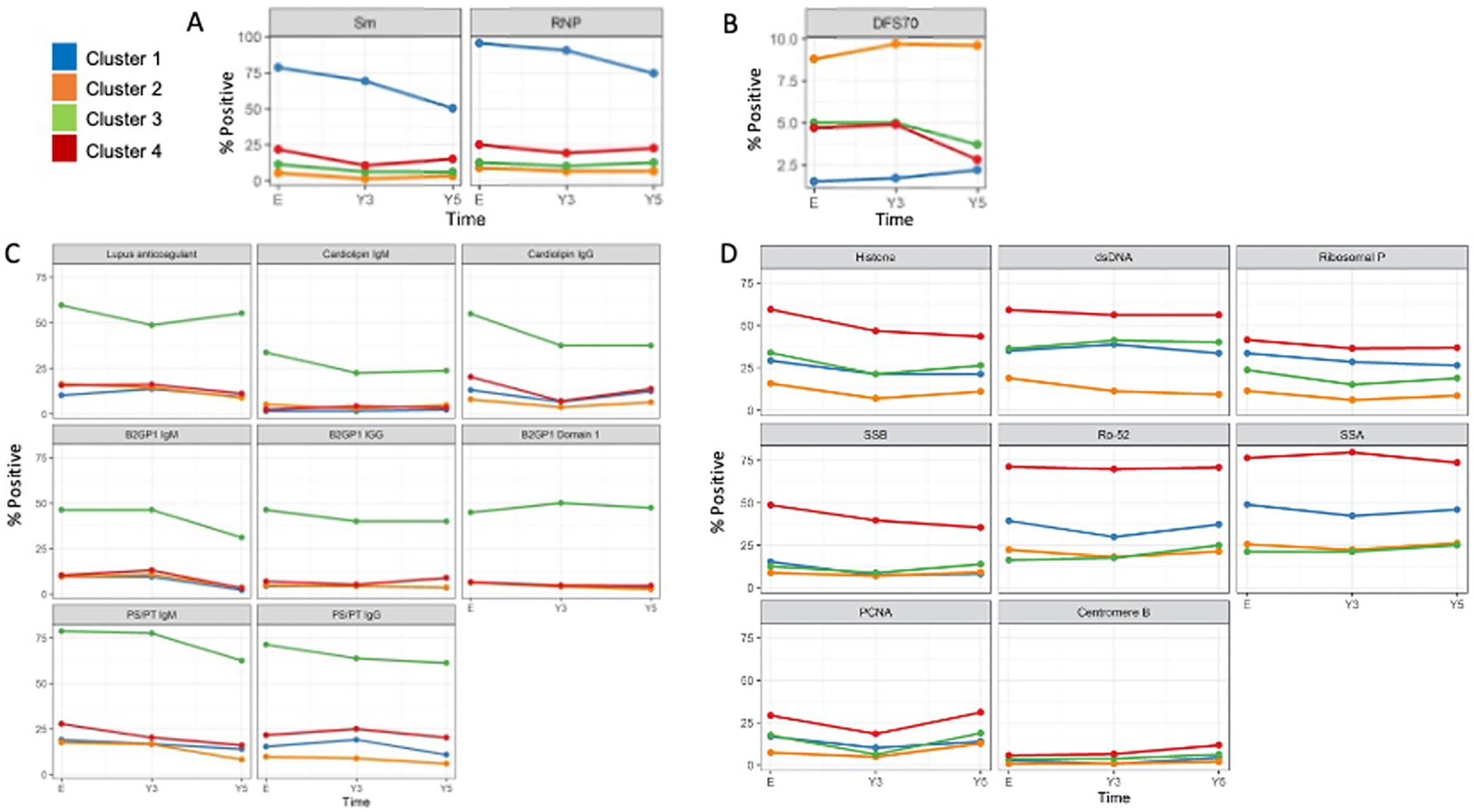
Cluster 1 (n=137, high frequency of anti-Smith, anti-U1RNP, AC-5 (large nuclear speckled pattern) and high ANA titres) had the highest cumulative disease activity and immunosuppressants/biologics use at year 10. Cluster 2 (n=376, low anti-double stranded DNA (dsDNA) and ANA titres) had the lowest disease activity, frequency of lupus nephritis and immunosuppressants/biologics use. Cluster 3 (n=80, highest frequency of all five antiphospholipid antibodies) had the highest frequency of seizures and hypocomplementaemia. Cluster 4 (n=212) also had high disease activity and was characterised by multiple autoantibody reactivity including to antihistone, anti-dsDNA, antiribosomal P, anti-Sjögren syndrome antigen A or Ro60, anti-Sjögren syndrome antigen B or La, anti-Ro52/Tripartite Motif Protein 21, antiproliferating cell nuclear antigen and anticentromere B). Clusters 1 (adjusted HR 2.60 (95% CI 1.12 to 6.05), p=0.03) and 3 (adjusted HR 2.87 (95% CI 1.22 to 6.74), p=0.02) had lower survival compared with cluster 2.
Four discrete SLE patient longitudinal autoantibody clusters were predictive of long-term disease activity, organ involvement, treatment requirements and mortality risk.
本研究应用一种新的纵向聚类技术,对来自大型、特征明确、多国初诊系统性红斑狼疮(SLE)队列的综合自身抗体数据进行分析,以确定预测临床结局的特征。
本研究纳入了 805 例 SLE 患者的人口统计学、临床和血清学数据,这些数据是在诊断后 15 个月内以及 3 年和 5 年随访时获得的。对于每次就诊,评估血清中 29 种抗核抗体(ANA)免疫荧光模式和 20 种自身抗体。基于主成分分析转换的纵向自身抗体谱的 K-均值聚类可识别离散的表型聚类。采用单因素方差分析比较 10 年随访时各聚类的入组人口统计学和临床结局。Cox 比例风险模型估计了疾病发病年龄调整后的生存风险比(HR)。
聚类 1(n=137,高频率的抗-Smith、抗-U1RNP、AC-5(大核斑点模式)和高 ANA 滴度)在第 10 年时具有最高的累积疾病活动度和免疫抑制剂/生物制剂使用率。聚类 2(n=376,低抗双链 DNA(dsDNA)和 ANA 滴度)具有最低的疾病活动度、狼疮肾炎发生率和免疫抑制剂/生物制剂使用率。聚类 3(n=80,五种抗磷脂抗体频率最高)癫痫发作和低补体血症发生率最高。聚类 4(n=212)也具有较高的疾病活动度,其特征是多种自身抗体反应性,包括抗组蛋白、抗 dsDNA、抗核糖体 P、抗 SS-A 或 Ro60、抗 SS-B 或 La、抗 Ro52/三结构域蛋白 21、抗增殖细胞核抗原和抗着丝粒 B)。聚类 1(调整后的 HR 2.60(95%CI 1.12 至 6.05),p=0.03)和 3(调整后的 HR 2.87(95%CI 1.22 至 6.74),p=0.02)与聚类 2 相比,生存率较低。
四个离散的 SLE 患者纵向自身抗体聚类可预测长期疾病活动度、器官受累、治疗需求和死亡风险。