Division of Tumor Biology & Immunology, Netherlands Cancer Institute, Amsterdam, The Netherlands.
Oncode Institute, Utrecht, The Netherlands.
Oncoimmunology. 2023 Apr 13;12(1):2201147. doi: 10.1080/2162402X.2023.2201147. eCollection 2023.
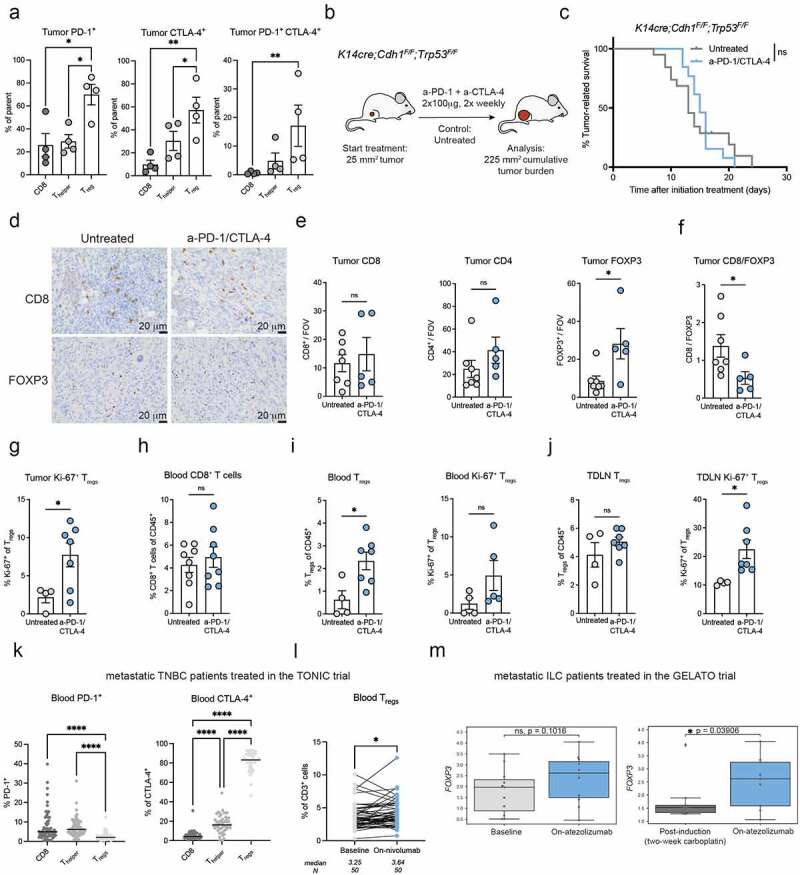
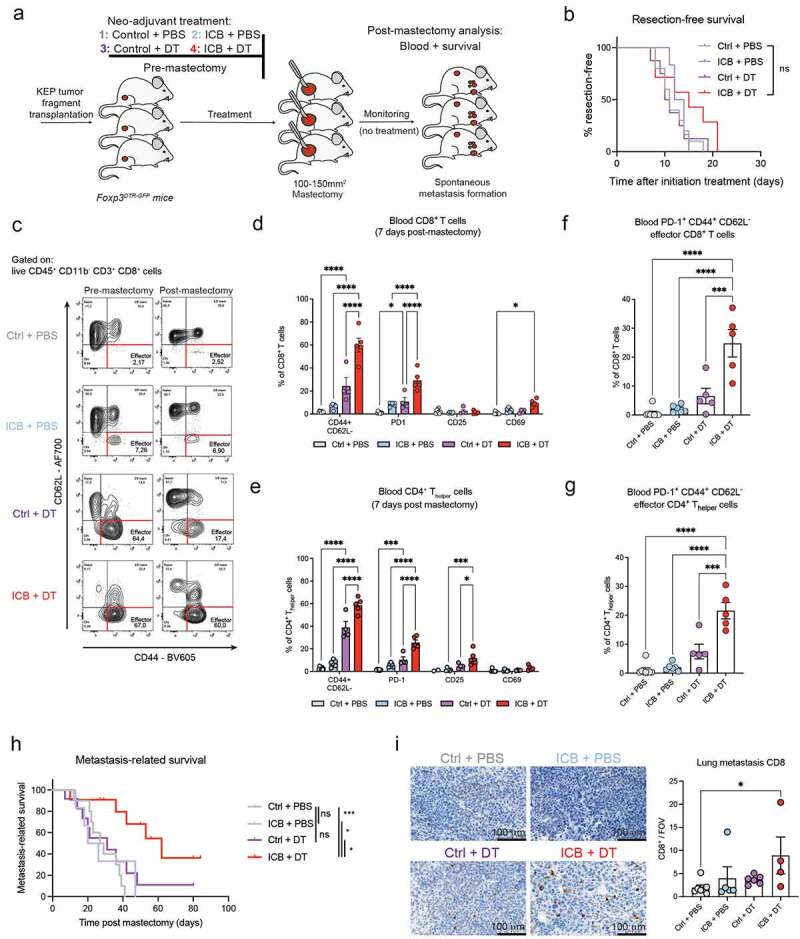
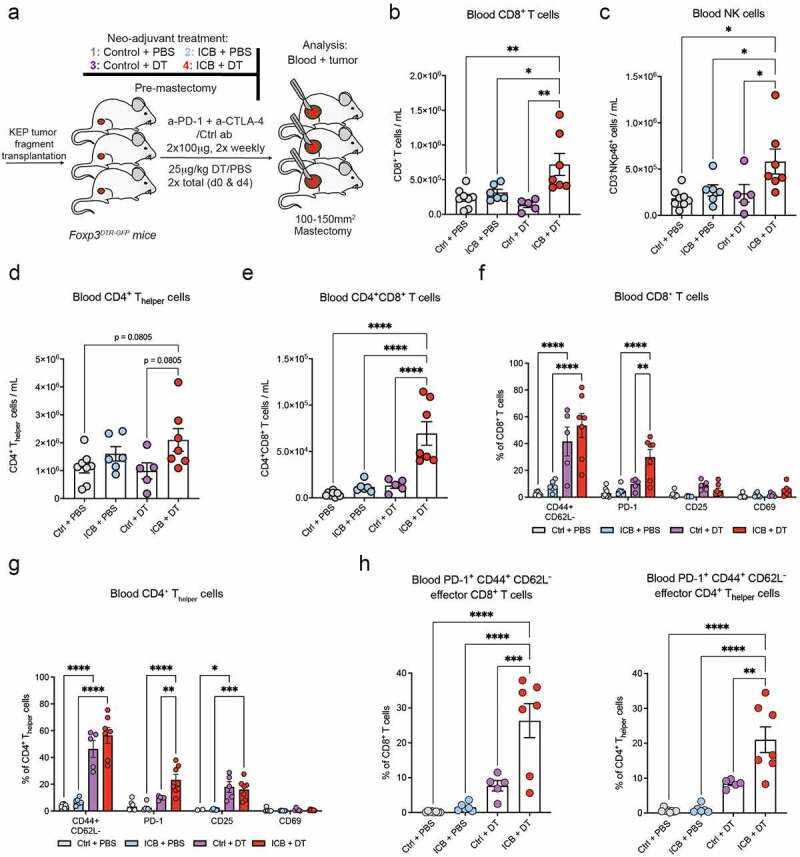
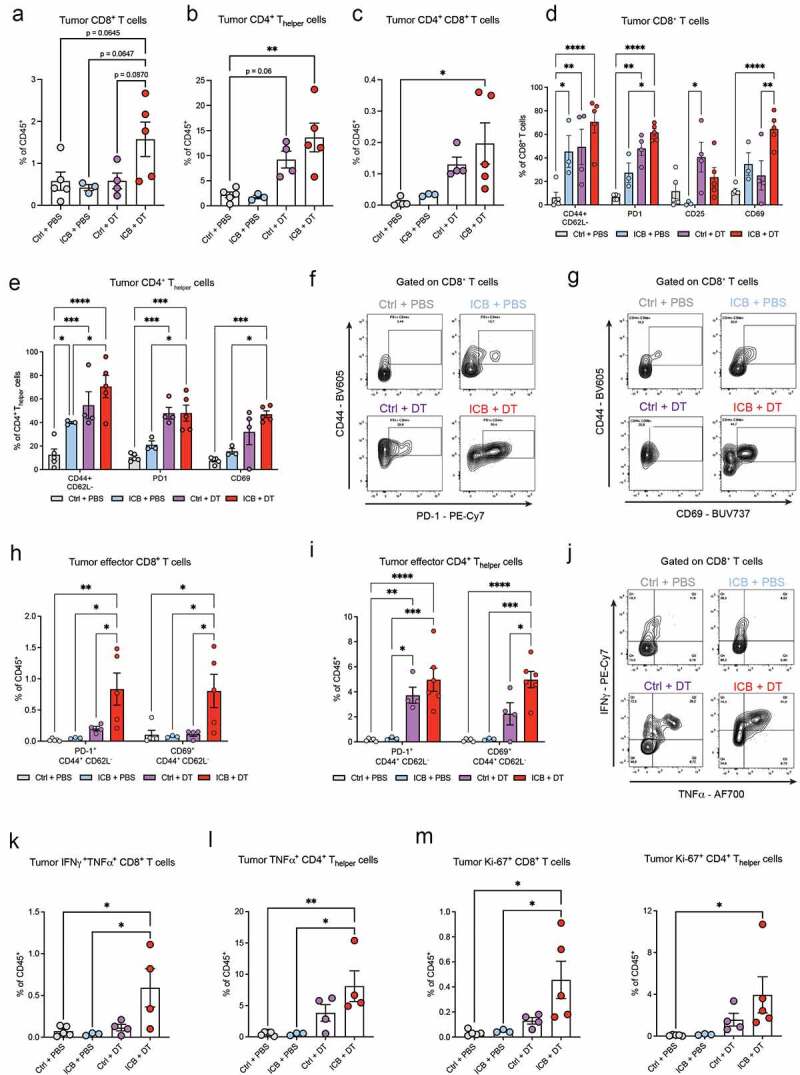
The clinical successes of immune checkpoint blockade (ICB) in advanced cancer patients have recently spurred the clinical implementation of ICB in the neoadjuvant and perioperative setting. However, how neoadjuvant ICB therapy affects the systemic immune landscape and metastatic spread remains to be established. Tumors promote both local and systemic expansion of regulatory T cells (T), which are key orchestrators of tumor-induced immunosuppression, contributing to immune evasion, tumor progression and metastasis. T express inhibitory immune checkpoint molecules and thus may be unintended targets for ICB therapy counteracting its efficacy. Using ICB-refractory models of spontaneous primary and metastatic breast cancer that recapitulate the poor ICB response of breast cancer patients, we observed that combined anti-PD-1 and anti-CTLA-4 therapy inadvertently promotes proliferation and activation of T in the tumor, tumor-draining lymph node and circulation. Also in breast cancer patients, T levels were elevated upon ICB. Depletion of T during neoadjuvant ICB in tumor-bearing mice not only reshaped the intratumoral immune landscape into a state favorable for ICB response but also induced profound and persistent alterations in systemic immunity, characterized by elevated CD8+ T cells and NK cells and durable T cell activation that was maintained after treatment cessation. While depletion of T in combination with neoadjuvant ICB did not inhibit primary tumor growth, it prolonged metastasis-related survival driven predominantly by CD8+ T cells. This study demonstrates that neoadjuvant ICB therapy of breast cancer can be empowered by simultaneous targeting of T extending metastasis-related survival, independent of a primary tumor response.
免疫检查点阻断(ICB)在晚期癌症患者中的临床成功最近促使 ICB 在新辅助和围手术期环境中的临床应用。然而,新辅助 ICB 治疗如何影响全身免疫景观和转移扩散仍有待确定。肿瘤促进调节性 T 细胞(T)的局部和全身扩张,T 是肿瘤诱导免疫抑制的关键协调者,导致免疫逃逸、肿瘤进展和转移。T 表达抑制性免疫检查点分子,因此可能是 ICB 治疗的意外靶点,从而降低其疗效。我们使用自发原发性和转移性乳腺癌的 ICB 难治性模型,这些模型再现了乳腺癌患者对 ICB 反应不良的情况,观察到联合抗 PD-1 和抗 CTLA-4 治疗无意中促进了 T 在肿瘤、肿瘤引流淋巴结和循环中的增殖和激活。同样在乳腺癌患者中,ICB 后 T 水平升高。在荷瘤小鼠的新辅助 ICB 期间耗尽 T,不仅重塑了有利于 ICB 反应的肿瘤内免疫景观,而且诱导了系统免疫的深刻和持久改变,表现为 CD8+T 细胞和 NK 细胞的升高和持久的 T 细胞激活,在治疗停止后仍能维持。虽然 T 的耗竭与新辅助 ICB 联合使用并没有抑制原发性肿瘤的生长,但它延长了转移相关的生存,主要由 CD8+T 细胞驱动。这项研究表明,新辅助 ICB 治疗乳腺癌可以通过同时靶向 T 来增强,从而延长转移相关的生存,而不依赖于原发性肿瘤的反应。