Surgical and Trauma Intensive Care Unit, Anesthesiology and Critical Care Department, Hôpital Pellegrin, CHU Bordeaux, Bordeaux University Hospital, Place Amélie Raba Léon, 33076, Bordeaux Cedex, France.
Anesthesiology and Critical Care Department, Clermont - Ferrand University Hospital, Clermont - Ferrand, France.
Crit Care. 2023 Apr 26;27(1):163. doi: 10.1186/s13054-023-04429-2.
The benefit-risk ratio of prophylactic non-invasive ventilation (NIV) and high-flow nasal oxygen therapy (HFNC-O) during the early stage of blunt chest trauma remains controversial because of limited data. The main objective of this study was to compare the rate of endotracheal intubation between two NIV strategies in high-risk blunt chest trauma patients.
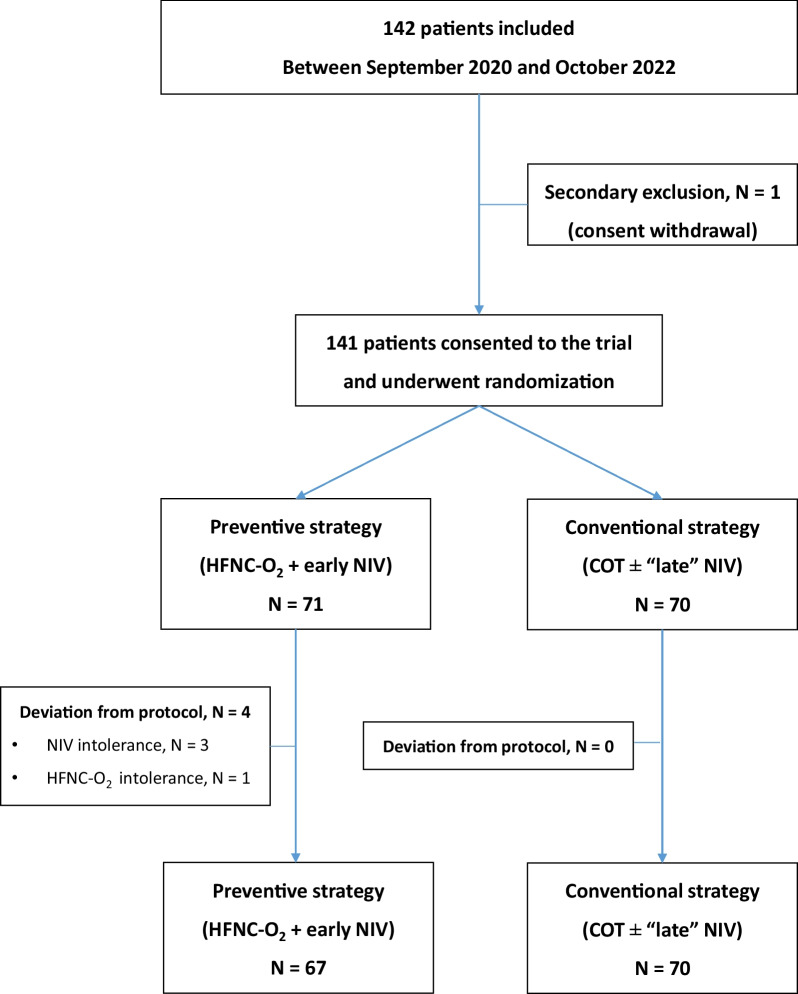
The OptiTHO trial was a randomized, open-label, multicenter trial over a two-year period. Every adult patients admitted in intensive care unit within 48 h after a high-risk blunt chest trauma (Thoracic Trauma Severity Score ≥ 8), an estimated PaO/FiO ratio < 300 and no evidence of acute respiratory failure were eligible for study enrollment (Clinical Trial Registration: NCT03943914). The primary objective was to compare the rate of endotracheal intubation for delayed respiratory failure between two NIV strategies: i) a prompt association of HFNC-O and "early" NIV in every patient for at least 48 h with vs. ii) the standard of care associating COT and "late" NIV, indicated in patients with respiratory deterioration and/or PaO/FiO ratio ≤ 200 mmHg. Secondary outcomes were the occurrence of chest trauma-related complications (pulmonary infection, delayed hemothorax or moderate-to-severe ARDS).
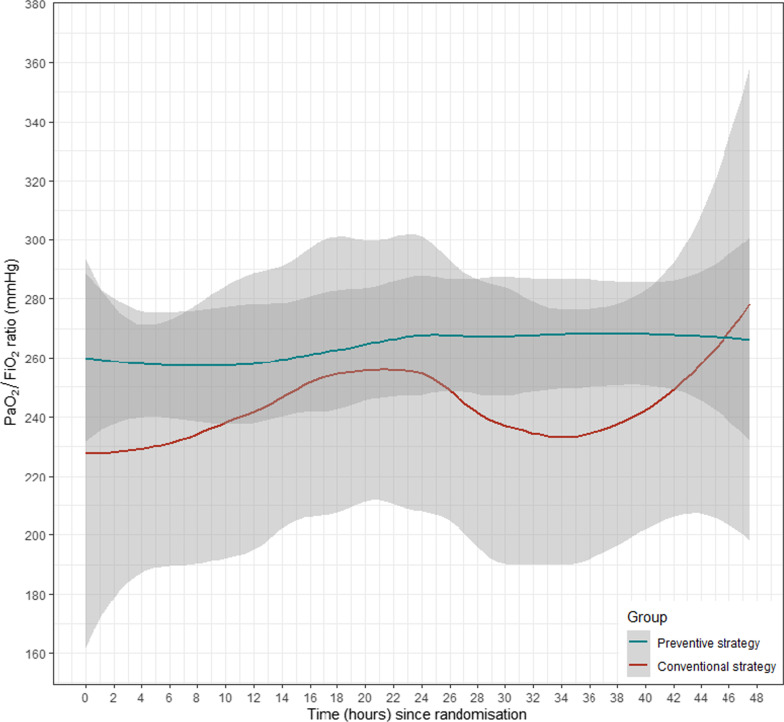
Study enrollment was stopped for futility after a 2-year study period and randomization of 141 patients. Overall, 11 patients (7.8%) required endotracheal intubation for delayed respiratory failure. The rate of endotracheal intubation was not significantly lower in patients treated with the experimental strategy (7% [5/71]) when compared to the control group (8.6% [6/70]), with an adjusted OR = 0.72 (95%IC: 0.20-2.43), p = 0.60. The occurrence of pulmonary infection, delayed hemothorax or delayed ARDS was not significantly lower in patients treated by the experimental strategy (adjusted OR = 1.99 [95%IC: 0.73-5.89], p = 0.18, 0.85 [95%IC: 0.33-2.20], p = 0.74 and 2.14 [95%IC: 0.36-20.77], p = 0.41, respectively).
A prompt association of HFNC-O with preventive NIV did not reduce the rate of endotracheal intubation or secondary respiratory complications when compared to COT and late NIV in high-risk blunt chest trauma patients with non-severe hypoxemia and no sign of acute respiratory failure.
NCT03943914, Registered 7 May 2019.
由于数据有限,预防性无创通气(NIV)和高流量鼻氧疗(HFNC-O)在钝性胸部创伤早期的获益-风险比仍存在争议。本研究的主要目的是比较两种 NIV 策略在高危钝性胸部创伤患者中的气管插管率。
OptiTHO 试验是一项为期两年的随机、开放标签、多中心试验。每例在高危钝性胸部创伤(创伤严重度评分≥8)后 48 小时内入住重症监护病房的成年患者,预计 PaO/FiO 比值<300,无急性呼吸衰竭证据,均符合研究纳入标准(临床试验注册:NCT03943914)。主要目的是比较两种 NIV 策略的气管插管率:i)每例患者均迅速联合 HFNC-O 和“早期”NIV 至少 48 小时,与 ii)标准治疗联合 COT 和“晚期”NIV,仅在呼吸恶化和/或 PaO/FiO 比值≤200mmHg 的患者中进行。次要结局是胸部创伤相关并发症(肺部感染、迟发性血胸或中重度 ARDS)的发生情况。
在为期两年的研究期间和对 141 名患者进行随机分组后,因无效性研究停止。总体而言,11 名患者(7.8%)因迟发性呼吸衰竭需要气管插管。与对照组(8.6%[6/70])相比,接受实验性治疗策略的患者气管插管率无显著降低(7%[5/71]),调整后的 OR=0.72(95%CI:0.20-2.43),p=0.60。接受实验性治疗策略的患者肺部感染、迟发性血胸或迟发性 ARDS 的发生率也无显著降低(调整后的 OR=1.99[95%CI:0.73-5.89],p=0.18,0.85[95%CI:0.33-2.20],p=0.74 和 2.14[95%CI:0.36-20.77],p=0.41)。
与 COT 和晚期 NIV 相比,在非严重低氧血症且无急性呼吸衰竭迹象的高危钝性胸部创伤患者中,HFNC-O 与预防性 NIV 的迅速联合并未降低气管插管率或继发性呼吸并发症的发生率。
NCT03943914,2019 年 5 月 7 日注册。