Department of Psychology, University of Liverpool, Liverpool, UK.
Department of Neurosurgery, The Walton Centre NHS Foundation Trust, Liverpool, UK.
BMC Musculoskelet Disord. 2023 Apr 27;24(1):333. doi: 10.1186/s12891-023-06446-2.
This study aimed to develop and externally validate prediction models of spinal surgery outcomes based on a retrospective review of a prospective clinical database, uniquely comparing multivariate regression and random forest (machine learning) approaches, and identifying the most important predictors.
Outcomes were change in back and leg pain intensity and Core Outcome Measures Index (COMI) from baseline to the last available postoperative follow-up (3-24 months), defined as minimal clinically important change (MCID) and continuous change score. Eligible patients underwent lumbar spine surgery for degenerative pathology between 2011 and 2021. Data were split by surgery date into development (N = 2691) and validation (N = 1616) sets for temporal external validation. Multivariate logistic and linear regression, and random forest classification and regression models, were fit to the development data and validated on the external data.
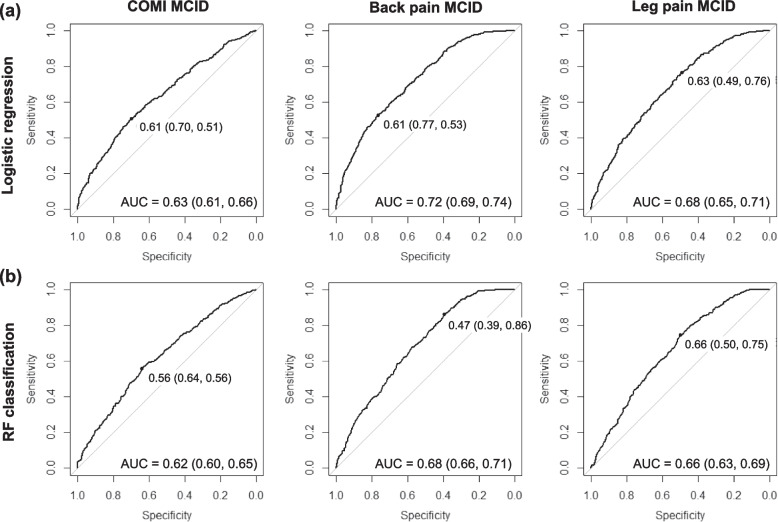
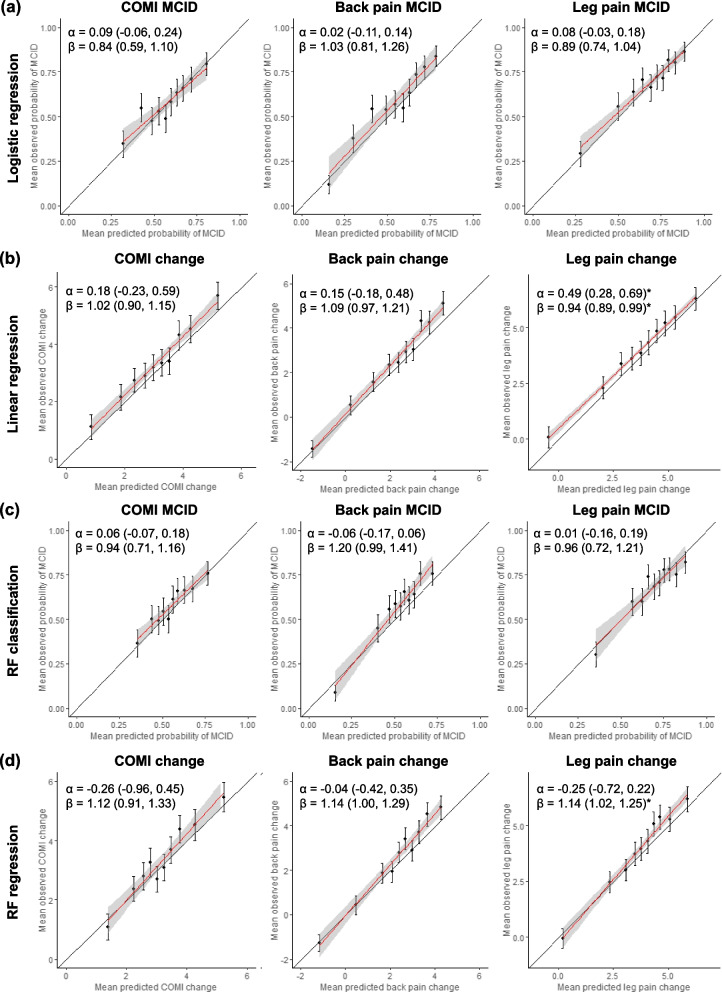
All models demonstrated good calibration in the validation data. Discrimination ability (area under the curve) for MCID ranged from 0.63 (COMI) to 0.72 (back pain) in regression, and from 0.62 (COMI) to 0.68 (back pain) in random forests. The explained variation in continuous change scores spanned 16%-28% in linear, and 15%-25% in random forests regression. The most important predictors included age, baseline scores on the respective outcome measures, type of degenerative pathology, previous spinal surgeries, smoking status, morbidity, and duration of hospital stay.
The developed models appear robust and generalisable across different outcomes and modelling approaches but produced only borderline acceptable discrimination ability, suggesting the need to assess further prognostic factors. External validation showed no advantage of the random forest approach.
本研究旨在基于前瞻性临床数据库的回顾性分析,开发和外部验证脊柱手术结果的预测模型,特别比较多元回归和随机森林(机器学习)方法,并确定最重要的预测因素。
结局是从基线到最后一次可获得的术后随访(3-24 个月)时背部和腿部疼痛强度以及核心结局测量指标(COMI)的变化,定义为最小临床重要变化(MCID)和连续变化评分。符合条件的患者在 2011 年至 2021 年间因退行性病变接受腰椎手术。根据手术日期将数据分为开发(N=2691)和验证(N=1616)数据集,进行时间外部验证。多元逻辑和线性回归以及随机森林分类和回归模型拟合于开发数据,并在外部数据上进行验证。
所有模型在验证数据中均表现出良好的校准能力。MCID 的判别能力(曲线下面积)在回归分析中从 COMI 的 0.63 到背痛的 0.72,在随机森林中从 COMI 的 0.62 到背痛的 0.68。线性模型中连续变化评分的解释方差为 16%-28%,随机森林回归模型为 15%-25%。最重要的预测因素包括年龄、各自结局测量的基线评分、退行性病变类型、以前的脊柱手术、吸烟状况、发病率和住院时间。
开发的模型似乎在不同的结局和建模方法中具有稳健性和可推广性,但产生的判别能力仅为边缘可接受,这表明需要进一步评估预后因素。外部验证表明随机森林方法没有优势。