J. Graham Brown Cancer Center, University of Louisville, Louisville, Kentucky, USA
Roswell Park Comprehensive Cancer Center, Buffalo, New York, USA.
J Immunother Cancer. 2023 May;11(5). doi: 10.1136/jitc-2022-006270.
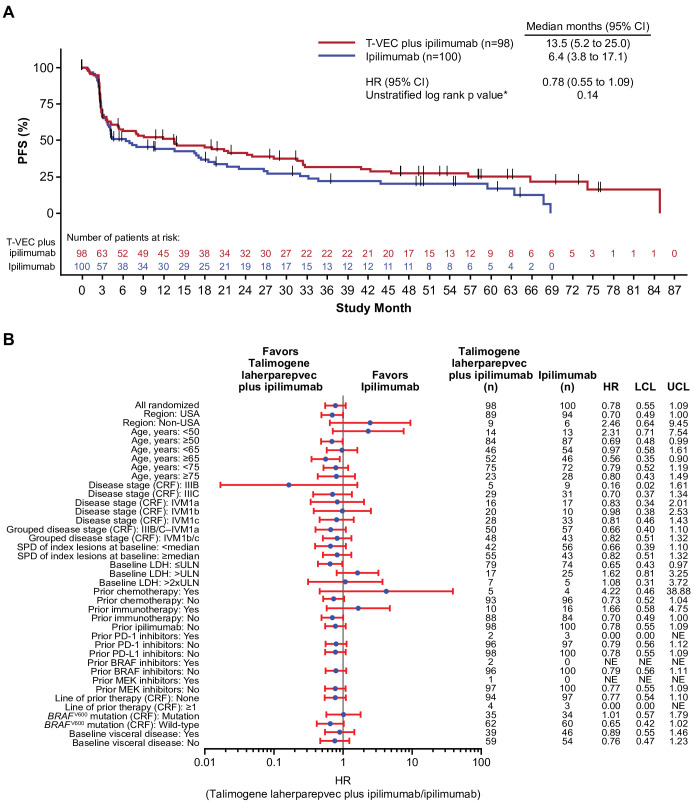
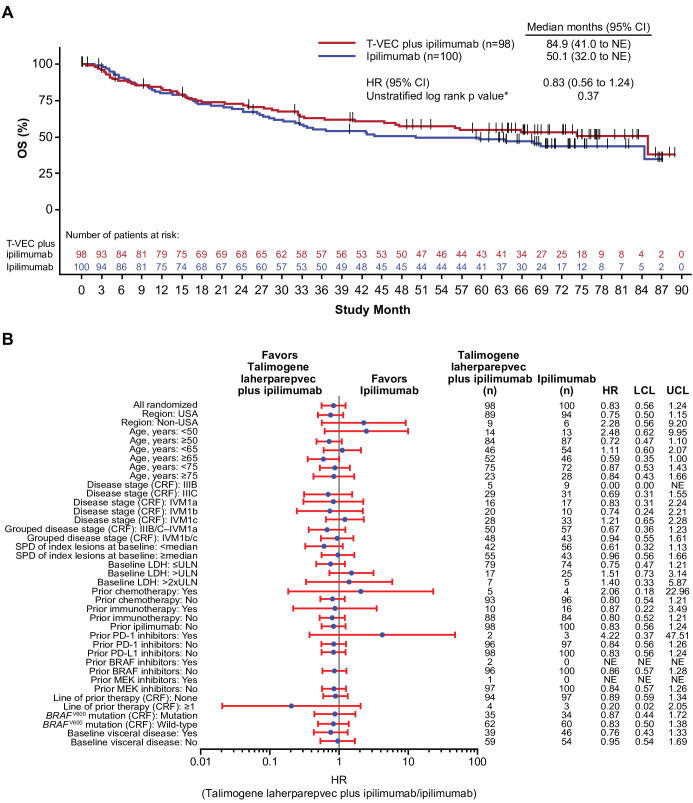
Talimogene laherparepvec (T-VEC) plus ipilimumab has demonstrated greater antitumor activity versus ipilimumab alone, without additional toxicity, in patients with advanced melanoma. Here, we report the 5-year outcomes from a randomized phase II study. These data provide the longest efficacy and safety follow-up for patients with melanoma treated with a combination of an oncolytic virus and a checkpoint inhibitor.Eligible patients with unresectable stage IIIB‒IV melanoma were randomized 1:1 to receive T-VEC plus ipilimumab or ipilimumab alone. T-VEC was administered intralesionally at 10 plaque-forming units (PFU)/mL in week 1, followed by 10 PFU/mL in week 4 and every 2 weeks thereafter. Ipilimumab (3 mg/kg every 3 weeks; ≤4 doses) was administered intravenously starting at week 1 in the ipilimumab arm and week 6 in the combination arm. The primary end point was investigator-assessed objective response rate (ORR) per immune-related response criteria; key secondary end points included durable response rate (DRR), duration of response (DOR), progression-free survival (PFS), overall survival (OS), and safety.Overall, 198 patients were randomized to receive the combination (n=98) or ipilimumab (n=100). The combination improved the ORR versus ipilimumab (35.7% vs 16.0%; OR 2.9; 95% CI 1.5 to 5.7; p=0.003). DRR was 33.7% and 13.0% (unadjusted OR 3.4; 95% CI 1.7 to 7.0; descriptive p=0.001), respectively. Among the objective responders, the median DOR was 69.2 months (95% CI 38.5 to not estimable) with the combination and was not reached with ipilimumab. Median PFS was 13.5 months with the combination and 6.4 months with ipilimumab (HR 0.78; 95% CI 0.55 to 1.09; descriptive p=0.14). Estimated 5-year OS was 54.7% (95% CI 43.9 to 64.2) in the combination arm and 48.4% (95% CI 37.9 to 58.1) in the ipilimumab arm. Forty-seven (48.0%) and 65 (65.0%) patients in the combination and ipilimumab arms, respectively, received subsequent therapies. No new safety signals were reported.At the 5-year follow-up, the improved response rates observed with T-VEC plus ipilimumab were durable. This is the first randomized controlled study of the combination of an oncolytic virus and a checkpoint inhibitor that meets its primary end point.Trial registration number: NCT01740297.
替莫唑胺(T-VEC)联合伊匹单抗在晚期黑色素瘤患者中表现出比单用伊匹单抗更大的抗肿瘤活性,且没有额外的毒性。在此,我们报告了一项随机的二期研究的 5 年结果。这些数据为接受溶瘤病毒和检查点抑制剂联合治疗的黑色素瘤患者提供了最长的疗效和安全性随访。
符合条件的无法切除的 IIIB-IV 期黑色素瘤患者按 1:1 随机接受 T-VEC 联合伊匹单抗或单用伊匹单抗治疗。T-VEC 在第 1 周以 10 个噬菌斑形成单位(PFU)/mL 剂量进行皮内注射,随后在第 4 周和此后每 2 周以 10 PFU/mL 剂量进行皮内注射。伊匹单抗(每 3 周 3mg/kg;最多 4 剂)在伊匹单抗组的第 1 周和联合组的第 6 周开始静脉内给药。主要终点是研究者评估的客观缓解率(ORR)根据免疫相关的反应标准;关键次要终点包括持久缓解率(DRR)、缓解持续时间(DOR)、无进展生存期(PFS)、总生存期(OS)和安全性。
总体而言,198 名患者被随机分配接受联合治疗(n=98)或伊匹单抗(n=100)。与伊匹单抗相比,联合治疗提高了 ORR(35.7% vs. 16.0%;OR 2.9;95%CI 1.5 至 5.7;p=0.003)。DRR 分别为 33.7%和 13.0%(未调整的 OR 3.4;95%CI 1.7 至 7.0;描述性 p=0.001)。在客观反应者中,联合组的中位 DOR 为 69.2 个月(95%CI 38.5 至无法估计),而伊匹单抗组未达到。联合组的中位 PFS 为 13.5 个月,伊匹单抗组为 6.4 个月(HR 0.78;95%CI 0.55 至 1.09;描述性 p=0.14)。联合组的 5 年 OS 估计为 54.7%(95%CI 43.9 至 64.2),伊匹单抗组为 48.4%(95%CI 37.9 至 58.1)。联合组和伊匹单抗组分别有 47(48.0%)和 65(65.0%)名患者接受了后续治疗。没有报告新的安全信号。
在 5 年随访时,T-VEC 联合伊匹单抗观察到的改善的缓解率是持久的。这是第一项符合主要终点的溶瘤病毒与检查点抑制剂联合治疗的随机对照研究。
NCT01740297。