Stroke Research Group and Division for Health & Social Care Research, Kings College London, London, UK.
Coalition of Stroke Taskforces for Stroke.
Int J Stroke. 2023 Oct;18(9):1084-1091. doi: 10.1177/17474930231177204. Epub 2023 May 30.
Prehospital care including recognition of stroke symptoms by the public and professionals combined with an efficient and effective emergency medical service (EMS) is essential to increase access to effective acute stroke care. We undertook a survey to document the status of stroke prehospital care globally.
A survey was distributed via email to the World Stroke Organization (WSO) members. Information was sought on the current status of stroke prehospital delay globally, including (1) ambulance availability and whether payment for use is required, (2) ambulance response times and the proportion of patients arriving at hospital by ambulance, (3) the proportion of patients arriving within 3 h and more than 24 h after symptom, (4) whether stroke care training of paramedics, call handlers, and primary care staff, (5) availability of specialist centers, and (6) the proportion of patients taken to specialist centers. Respondents were also asked to identify the top three changes in prehospital care that would benefit their population. Data were analyzed descriptively at both country and continent level.
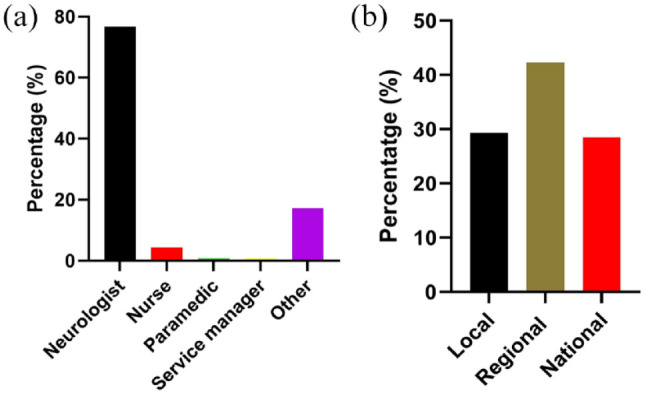
Responses were received from 116 individuals in 43 countries, with a response rate of 4.7%. Most respondents (90%) reported access to ambulances, but 40% of respondents reported payment was required by the patient. Where an ambulance service was available (105 respondents) 37% of respondents reported that less than 50% of patients used an ambulance and 12% less than 20% of patients used an ambulance. Large variations in ambulance response times were reported both within and between countries. Most of the participating high-income countries (HIC) offered a service used by patients, but this was rarely the case for the low- and middle-income countries (LMIC). Time to admission was often much longer in LMIC, and there was less access to stroke training for EMS and primary care staff.
Significant deficiencies in stroke prehospital care exist globally especially in LMIC. In all countries, there are opportunities to improve the quality of the service in ways that would likely result in improved outcomes after acute stroke.
包括公众和专业人士识别中风症状的院前护理,以及高效、有效的紧急医疗服务(EMS),对于增加获得有效急性中风护理的机会至关重要。我们进行了一项调查,以记录全球中风院前护理的现状。
通过电子邮件向世界中风组织(WSO)成员分发了一份调查问卷。调查内容包括全球中风院前延迟的现状,包括:(1)救护车的可用性以及使用是否需要付费;(2)救护车响应时间以及乘坐救护车到医院的患者比例;(3)症状出现后 3 小时内和 24 小时以上到达的患者比例;(4)是否对护理人员、接线员和初级保健人员进行中风护理培训;(5)是否有专门中心;以及(6)患者送往专门中心的比例。受访者还被要求确定对其人群最有益的院前护理三个变化。对国家和大陆层面的数据进行了描述性分析。
共收到来自 43 个国家的 116 名个人的回复,回复率为 4.7%。大多数受访者(90%)表示可以获得救护车,但 40%的受访者表示患者需要付费。在有救护车服务的情况下(105 名受访者),37%的受访者报告称,只有不到 50%的患者使用救护车,12%的受访者不到 20%的患者使用救护车。在国家内部和国家之间,救护车响应时间差异很大。大多数参与的高收入国家(HIC)都提供了患者使用的服务,但在低收入和中等收入国家(LMIC)很少有这种情况。在 LMIC,入院时间往往要长得多,并且 EMS 和初级保健人员获得中风培训的机会也较少。
全球范围内,尤其是在 LMIC,中风院前护理存在重大缺陷。在所有国家,都有机会以可能改善急性中风后结果的方式提高服务质量。