Sveikata Lukas, Melaika Kazimieras, Wiśniewski Adam, Vilionskis Aleksandras, Petrikonis Kȩstutis, Stankevičius Edgaras, Jurjans Kristaps, Ekkert Aleksandra, Jatužis Dalius, Masiliūnas Rytis
J. Philip Kistler Stroke Research Center, Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States.
Institute of Cardiology, Medical Academy, Lithuanian University of Health Sciences, Kaunas, Lithuania.
Front Neurol. 2022 Apr 7;13:765165. doi: 10.3389/fneur.2022.765165. eCollection 2022.
Acute stroke treatment outcomes are predicated on reperfusion timeliness which can be improved by better prehospital stroke identification. We aimed to assess the effect of interactive emergency medical services (EMS) training on stroke recognition and prehospital care performance in a very high-risk cardiovascular risk population in Lithuania.
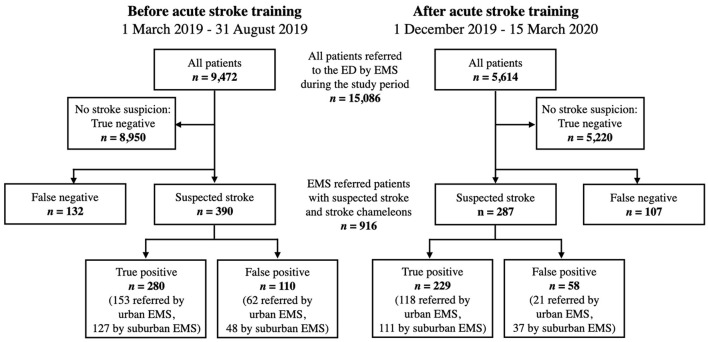
We conducted a single-center interrupted time-series study between March 1, 2019 and March 15, 2020. Two-hour small-group interactive stroke training sessions were organized for 166 paramedics serving our stroke network. We evaluated positive predictive value (PPV) and sensitivity for stroke including transient ischemic attack identification, onset-to-door time, and hospital-based outcomes during 6-months prior and 3.5 months after the training. The study outcomes were compared between EMS providers in urban and suburban areas.
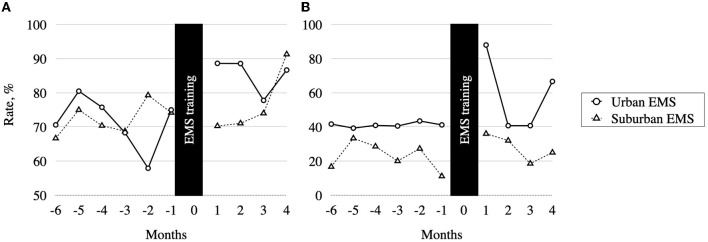
In total, 677 suspected stroke cases and 239 stroke chameleons (median age 75 years, 54.8% women) were transported by EMS. After the training, we observed improved PPV for stroke recognition (79.8% . 71.8%, = 0.017) and a trend of decreased in-hospital mortality (7.8% . 12.3, = 0.070). Multivariable logistic regression models adjusted for age, gender, EMS location, and stroke subtype showed an association between EMS stroke training and improved odds of stroke identification (adjusted odds ratio [aOR] 1.6 [1.1-2.3]) and onset-to-door ≤ 90 min (aOR 1.6 [1.1-2.5]). The improvement of PPV was observed in urban EMS (84.9% . 71.2%, = 0.003), but not in the suburban group (75.0% . 72.6%, = 0.621).
The interactive EMS training was associated with a robust improvement of stroke recognition, onset to hospital transport time, and a trend of decreased in-hospital mortality. Adapted training strategies may be needed for EMS providers in suburban areas. Future studies should evaluate the long-term effects of the EMS training and identify optimal retraining intervals.
急性卒中的治疗效果取决于再灌注的及时性,而更好的院前卒中识别可改善这一点。我们旨在评估互动式紧急医疗服务(EMS)培训对立陶宛心血管风险极高人群中卒中识别及院前护理表现的影响。
我们在2019年3月1日至2020年3月15日期间进行了一项单中心中断时间序列研究。为服务于我们卒中网络的166名护理人员组织了为期两小时的小组互动式卒中培训课程。我们评估了卒中的阳性预测值(PPV)和敏感性,包括短暂性脑缺血发作的识别、发病至入院时间以及培训前6个月和培训后3.5个月期间基于医院的结局。对城市和郊区的EMS提供者的研究结果进行了比较。
EMS共运送了677例疑似卒中病例和239例卒中变色龙患者(中位年龄75岁,女性占54.8%)。培训后,我们观察到卒中识别的PPV有所改善(79.8%对71.8%,P = 0.017),且院内死亡率有下降趋势(7.8%对12.3%,P = 0.070)。对年龄、性别、EMS地点和卒中亚型进行调整的多变量逻辑回归模型显示,EMS卒中培训与卒中识别几率的提高(调整后的优势比[aOR]为1.6[1.1 - 2.3])以及发病至入院时间≤90分钟(aOR为1.6[1.1 - 2.5])之间存在关联。在城市EMS中观察到PPV有所改善(84.9%对71.2%,P = 0.003),但在郊区组中未观察到改善(75.0%对72.6%,P = 0.621)。
互动式EMS培训与卒中识别、发病至医院转运时间的显著改善以及院内死亡率下降趋势相关。郊区的EMS提供者可能需要采用适应性培训策略。未来的研究应评估EMS培训的长期效果并确定最佳再培训间隔。