Department of Hematology and Oncology, University Hospital Muenster, Muenster, Germany.
European Society for Blood and Marrow Transplantation, Hôpital St. Antoine, Paris, France.
Leukemia. 2023 Jul;37(7):1511-1520. doi: 10.1038/s41375-023-01924-x. Epub 2023 May 8.
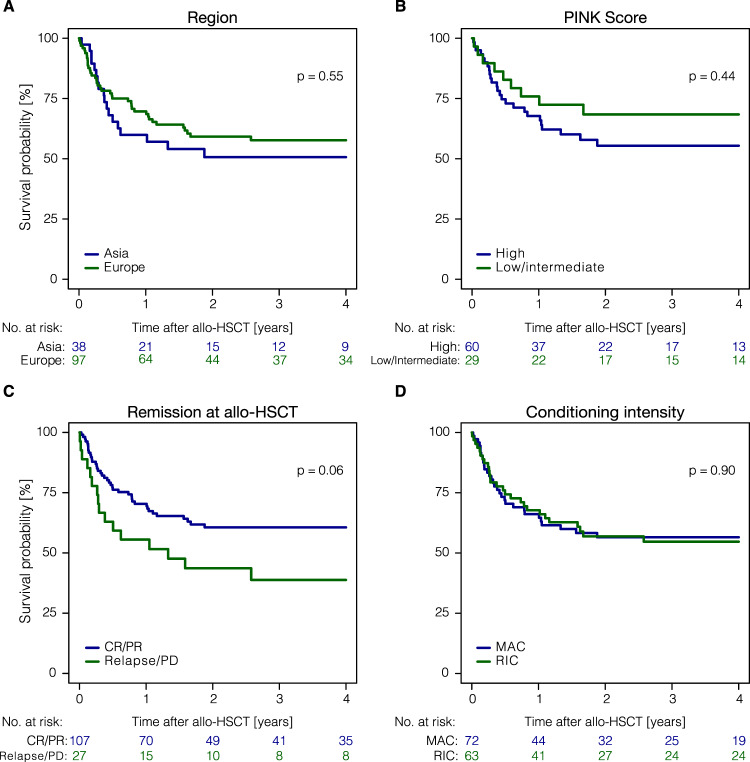
Natural killer/T-cell lymphomas (NKTCL) represent rare and aggressive lymphoid malignancies. Patients (pts) with relapsed/refractory disease after Asparaginase (ASPA)-based chemotherapy have a dismal prognosis. To better define the role of allogeneic hematopoietic stem cell transplantation (allo-HSCT), we conducted a retrospective analysis of data shared with the European Society for Blood and Marrow Transplantation (EBMT) and cooperating Asian centers. We identified 135 pts who received allo-HSCT between 2010 and 2020. Median age was 43.4 years at allo-HSCT, 68.1% were male. Ninety-seven pts (71.9 %) were European, 38 pts (28.1%) Asian. High Prognostic Index for NKTCL (PINK) scores were reported for 44.4%; 76.3% had >1 treatment, 20.7% previous auto-HSCT, and 74.1% ASPA-containing regimens prior to allo-HSCT. Most (79.3%) pts were transplanted in CR/PR. With a median follow-up of 4.8 years, 3-year progression-free(PFS) and overall survival were 48.6% (95%-CI:39.5-57%) and 55.6% (95%-CI:46.5-63.8%). Non-relapse mortality at 1 year was 14.8% (95%-CI:9.3-21.5%) and 1-year relapse incidence 29.6% (95%-CI:21.9-37.6%). In multivariate analyses, shorter time interval (0-12 months) between diagnosis and allo-HSCT [HR = 2.12 (95%-CI:1.03-4.34); P = 0.04] and transplantation not in CR/PR [HR = 2.20 (95%-CI:0.98-4.95); P = 0.056] reduced PFS. Programmed cell death protein 1(PD-1/PD-L1) treatment before HSCT neither increased GVHD nor impacted survival. We demonstrate that allo-HSCT can achieve long-term survival in approximately half of pts allografted for NKTCL.
自然杀伤/T 细胞淋巴瘤(NKTCL)是一种罕见且侵袭性的淋巴恶性肿瘤。接受基于天冬酰胺酶(ASPA)的化疗后复发/难治的患者预后极差。为了更好地定义异基因造血干细胞移植(allo-HSCT)的作用,我们对与欧洲血液和骨髓移植学会(EBMT)及合作亚洲中心共享的数据进行了回顾性分析。我们共纳入 135 例于 2010 年至 2020 年间接受 allo-HSCT 的患者。allo-HSCT 时的中位年龄为 43.4 岁,68.1%为男性。97 例(71.9%)为欧洲人,38 例(28.1%)为亚洲人。44.4%的患者报告有高 NKTCL 预后指数(PINK)评分;76.3%的患者接受过 1 次以上治疗,20.7%的患者接受过自体 HSCT,74.1%的患者在 allo-HSCT 前接受了包含 ASPA 的方案。大多数(79.3%)患者在完全缓解/部分缓解(CR/PR)时接受移植。中位随访 4.8 年后,3 年无进展生存(PFS)和总生存(OS)率分别为 48.6%(95%CI:39.5-57%)和 55.6%(95%CI:46.5-63.8%)。1 年非复发死亡率为 14.8%(95%CI:9.3-21.5%),1 年复发率为 29.6%(95%CI:21.9-37.6%)。多因素分析显示,诊断与 allo-HSCT 之间的时间间隔较短(0-12 个月)[HR=2.12(95%CI:1.03-4.34);P=0.04],allo-HSCT 未达到 CR/PR[HR=2.20(95%CI:0.98-4.95);P=0.056]会降低 PFS。HSCT 前接受程序性细胞死亡蛋白 1(PD-1/PD-L1)治疗既不会增加移植物抗宿主病(GVHD),也不会影响生存。我们证明,allo-HSCT 可以使大约一半接受 NKTCL 移植的患者获得长期生存。