Wang Justin Z, Landry Alexander P, Nassiri Farshad, Merali Zamir A, Patel Zeel, Lee Grace, Rogers Lauren, Zuccato Jeffrey A, Voisin Mathew R, Munoz David, Tsang Derek S, Laperriere Normand, Zadeh Gelareh
MacFeeters Hamilton Neuro-Oncology Program, Princess Margaret Cancer Centre, University Health Network and University of Toronto, ON, Canada.
Division of Neurosurgery, Department of Surgery, University of Toronto, Toronto, ON, Canada.
Clin Transl Radiat Oncol. 2023 Apr 24;41:100631. doi: 10.1016/j.ctro.2023.100631. eCollection 2023 Jul.
Surgery is the primary treatment for most meningiomas. However, primary fractionated radiotherapy (fRT) remains an option for patients with larger meningiomas in challenging anatomic locations or patients at prohibitively high surgical risk. Outcome prediction for these patients is uncertain and cannot be guided by histopathology without available tumor tissue from surgery. Therefore, we aimed to assess the clinical factors that contribute to treatment failure in a large cohort of meningiomas consecutively treated with fRT as primary therapy, with the goal of identifying predictors of response.
Patients treated with primary fRT for intracranial meningiomas from 1998 to 2017 were reviewed. Those who received primary surgical resection, radiosurgery, previous fRT, or had <6 months of clinical follow-up were excluded. We applied logistic regression and Cox regression modeling to ascertain key predictors of treatment failure, progression-free survival (PFS), and adverse events (AE) following fRT.
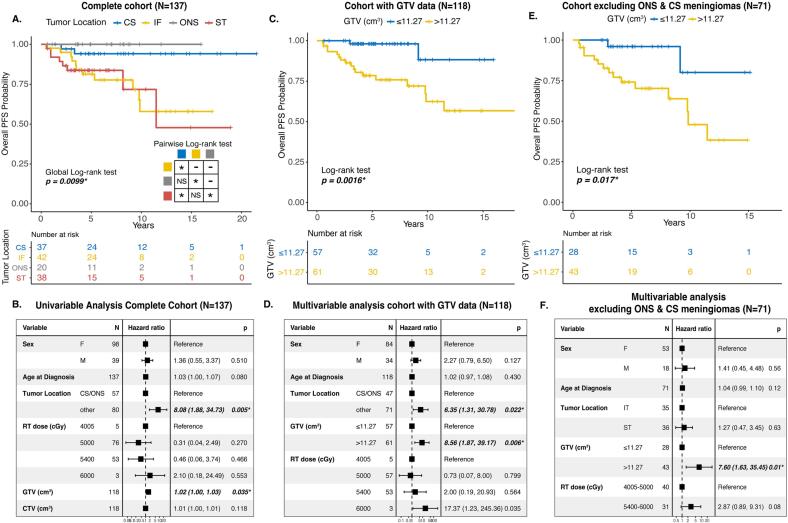
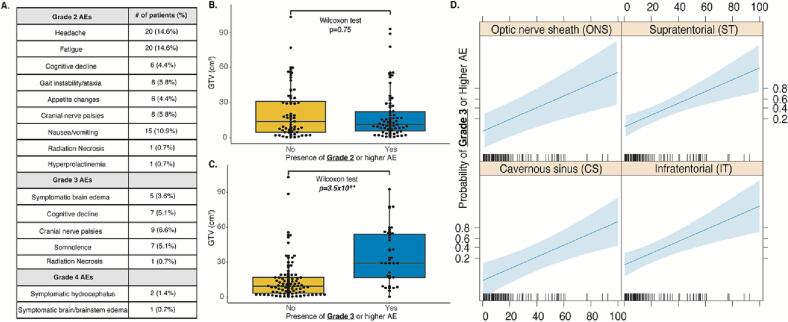
Our cohort included 137 meningiomas, 21 of which progressed after fRT (median PFS 3.45 years). Progressive meningiomas had a larger median gross tumor volume (GTV) compared to those that remained stable (19.1 cm vs 9.6 cm, p = 2.86 × 10). GTV > 11.27 cm was independently predictive of progression and larger GTV was associated with higher risk of significant (grades 3/4) AE following fRT. Cavernous sinus and optic nerve sheath meningiomas had overall excellent outcomes post-fRT.
We present a large cohort of meningiomas treated with primary fRT and find GTV and anatomic location to be key predictors of outcome, adding to the complex treatment considerations for this heterogeneous disease.
手术是大多数脑膜瘤的主要治疗方法。然而,对于解剖位置具有挑战性的较大脑膜瘤患者或手术风险极高的患者,原发性分次放疗(fRT)仍是一种选择。这些患者的预后预测尚不确定,且在没有手术获取的肿瘤组织的情况下,无法通过组织病理学进行指导。因此,我们旨在评估在一大群接受fRT作为主要治疗的脑膜瘤患者中导致治疗失败的临床因素,目标是确定反应的预测因素。
回顾了1998年至2017年接受原发性fRT治疗颅内脑膜瘤的患者。排除那些接受过原发性手术切除、放射外科手术、既往fRT或临床随访时间<6个月的患者。我们应用逻辑回归和Cox回归模型来确定fRT后治疗失败、无进展生存期(PFS)和不良事件(AE)的关键预测因素。
我们的队列包括137例脑膜瘤,其中21例在fRT后进展(中位PFS 3.45年)。与保持稳定的脑膜瘤相比,进展性脑膜瘤的中位肿瘤总体积(GTV)更大(19.1 cm对9.6 cm,p = 2.86×10)。GTV>11.27 cm可独立预测进展,且较大的GTV与fRT后发生严重(3/4级)AE的较高风险相关。海绵窦和视神经鞘脑膜瘤在fRT后的总体预后良好。
我们展示了一大群接受原发性fRT治疗的脑膜瘤患者,并发现GTV和解剖位置是预后的关键预测因素,这为这种异质性疾病的复杂治疗考虑增添了内容。