Department of Radiology, University Hospital, LMU Munich, Marchioninistr. 15, 81377, Munich, Germany.
Laboratory for Translational Cancer Immunology, Gene Center of the LMU Munich, Munich, Germany.
Cancer Imaging. 2023 May 15;23(1):44. doi: 10.1186/s40644-023-00566-7.
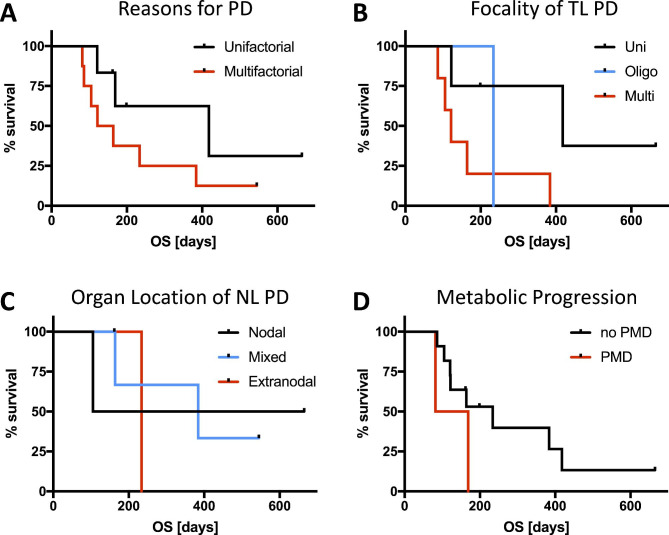
Chimeric antigen receptor T-cell therapy (CART) prolongs survival for patients with refractory or relapsed lymphoma. Discrepancies among different response criteria for lymphoma under CART were recently shown. Our objective was to evaluate reasons for discordance among different response criteria and their relation to overall survival.
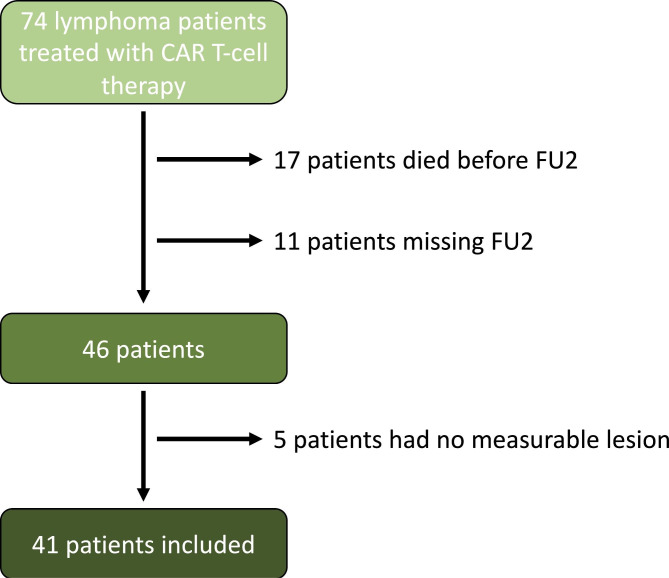
Consecutive patients with baseline and follow-up imaging at 30 (FU1) and 90 days (FU2) after CART were included. Overall response was determined based on Lugano, Cheson, response evaluation criteria in lymphoma (RECIL) and lymphoma response to immunomodulatory therapy criteria (LYRIC). Overall response rate (ORR) and rates of progressive disease (PD) were determined. For each criterion reasons for PD were analyzed in detail.
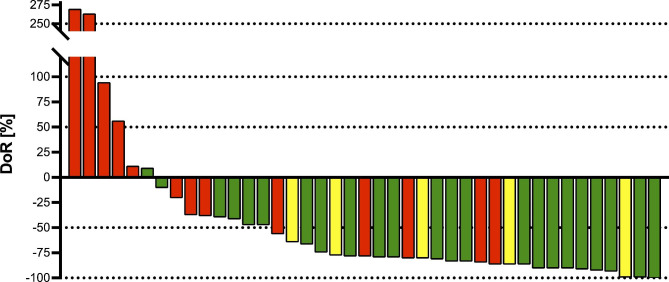
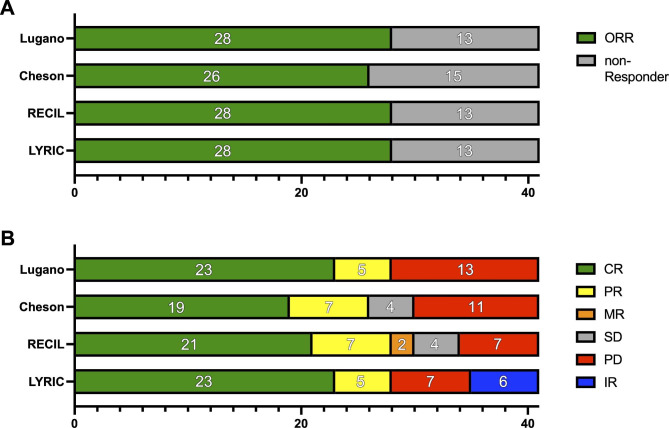
41 patients were included. ORR was 68%, 68%, 63%, and 68% at FU2 by Lugano, Cheson, RECIL, and LYRIC, respectively. PD rates differed among criteria with 32% by Lugano, 27% by Cheson, 17% by RECIL, and 17% by LYRIC. Dominant reasons for PD according to Lugano were target lesion (TL) progression (84.6%), new appearing lesions (NL; 53.8%), non-TL progression (27.3%), and progressive metabolic disease (PMD; 15.4%). Deviations among the criteria for defining PD were largely explained by PMD of preexisting lesions that are defined as PD only by Lugano and non-TL progression, which is not defined as PD by RECIL and in some cases classified as indeterminate response by LYRIC.
Following CART, lymphoma response criteria show differences in imaging endpoints, especially in defining PD. The response criteria must be considered when interpreting imaging endpoints and outcomes from clinical trials.
嵌合抗原受体 T 细胞疗法(CART)可延长复发或难治性淋巴瘤患者的生存期。最近显示,CART 下淋巴瘤的不同反应标准之间存在差异。我们的目的是评估不同反应标准之间差异的原因及其与总生存期的关系。
连续纳入基线和 CART 后 30 天(FU1)和 90 天(FU2)随访成像的患者。根据 Lugano、Cheson、淋巴瘤反应评估标准(RECIL)和淋巴瘤免疫调节治疗反应标准(LYRIC)确定总反应。确定总缓解率(ORR)和进展性疾病(PD)率。详细分析了每个标准中 PD 的原因。
共纳入 41 例患者。FU2 时 Lugano、Cheson、RECIL 和 LYRIC 的 ORR 分别为 68%、68%、63%和 68%。根据 Lugano,PD 率在标准之间存在差异,为 32%;Cheson 为 27%;RECIL 为 17%;LYRIC 为 17%。根据 Lugano,PD 的主要原因是靶病灶(TL)进展(84.6%)、新出现病灶(NL;53.8%)、非-TL 进展(27.3%)和进行性代谢疾病(PMD;15.4%)。定义 PD 的标准之间的差异主要由先前存在的病变的 PMD 解释,仅 Lugano 将其定义为 PD,而非 TL 进展在 RECIL 中不被定义为 PD,在某些情况下,LYRIC 将其归类为不确定反应。
CART 后,淋巴瘤反应标准在影像学终点方面存在差异,尤其是在定义 PD 方面。在解释影像学终点和临床试验结果时,必须考虑反应标准。