Department of Medicine III, Hematology and Oncology, University Hospital, LMU Munich, Munich, Germany.
Laboratory for Translational Cancer Immunology, LMU Gene Center, Munich, Germany.
J Immunother Cancer. 2022 May;10(5). doi: 10.1136/jitc-2021-004475.
CD19-directed chimeric antigen receptor T-cell therapy (CAR-T) represents a promising treatment modality for an increasing number of B-cell malignancies. However, prolonged cytopenias and infections substantially contribute to the toxicity burden of CAR-T. The recently developed CAR-HEMATOTOX (HT) score-composed of five pre-lymphodepletion variables (eg, absolute neutrophil count, platelet count, hemoglobin, C-reactive protein, ferritin)-enables risk stratification of hematological toxicity.
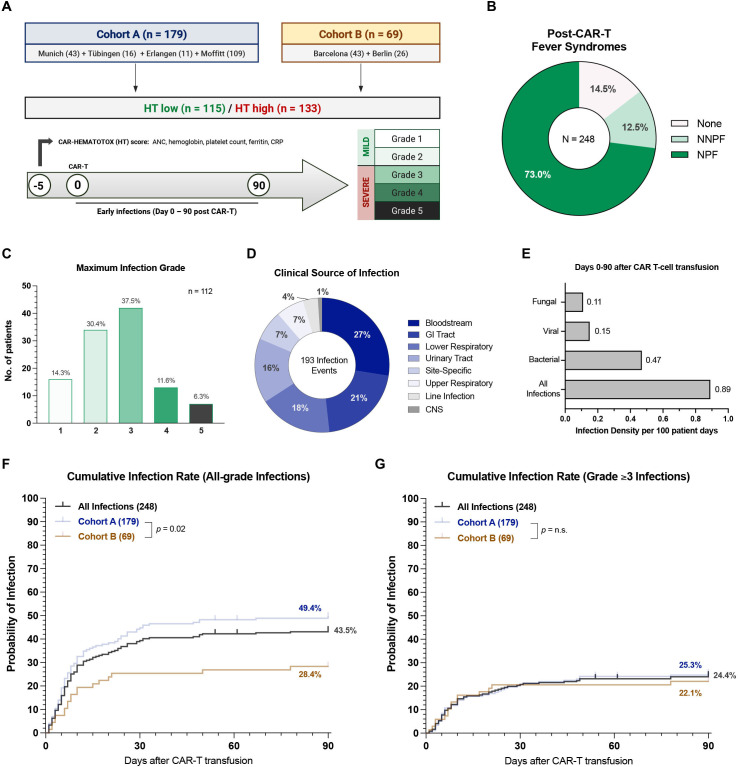
In this multicenter retrospective analysis, we characterized early infection events (days 0-90) and clinical outcomes in 248 patients receiving standard-of-care CD19 CAR-T for relapsed/refractory large B-cell lymphoma. This included a derivation cohort (cohort A, 179 patients) and a second independent validation cohort (cohort B, 69 patients). Cumulative incidence curves were calculated for all-grade, grade ≥3, and specific infection subtypes. Clinical outcomes were studied via Kaplan-Meier estimates.
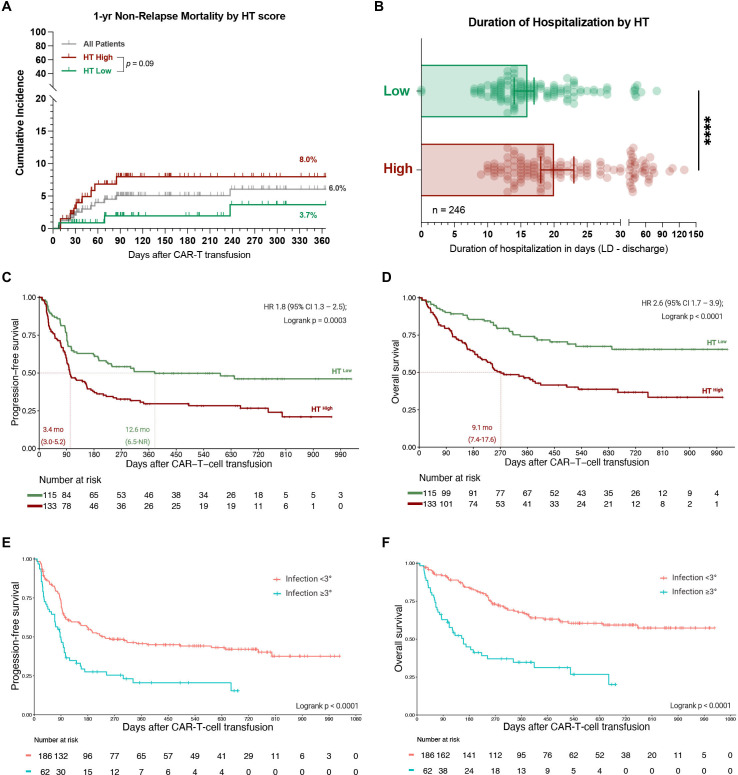
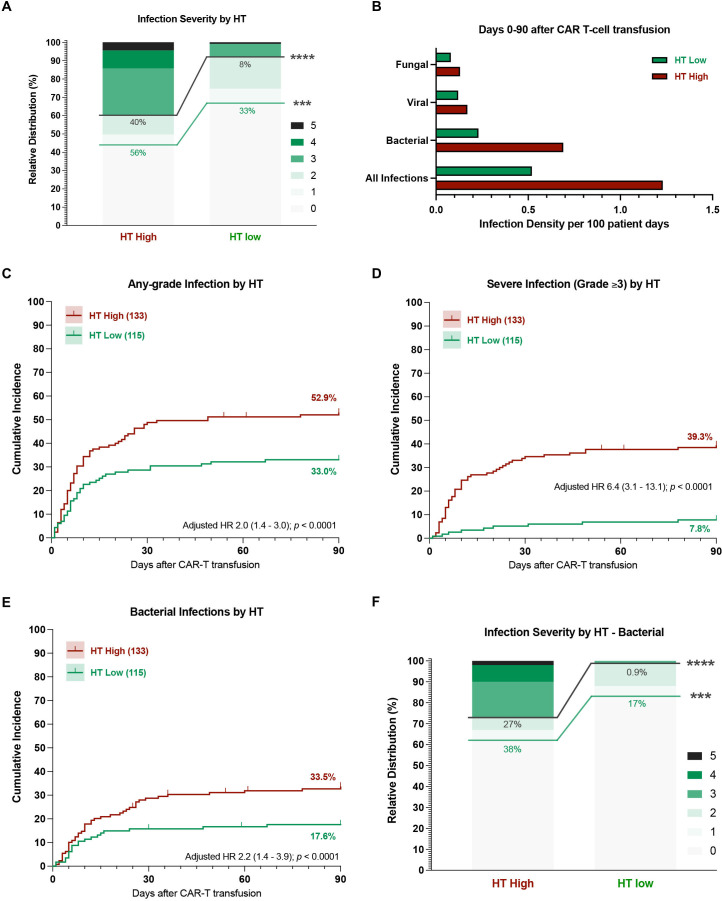
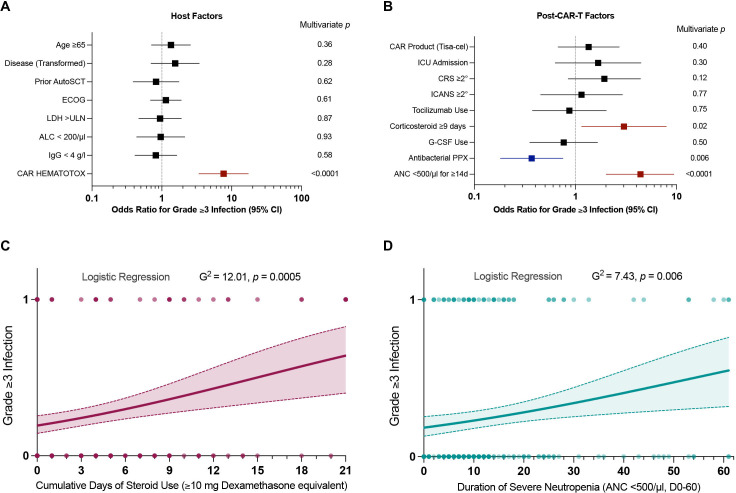
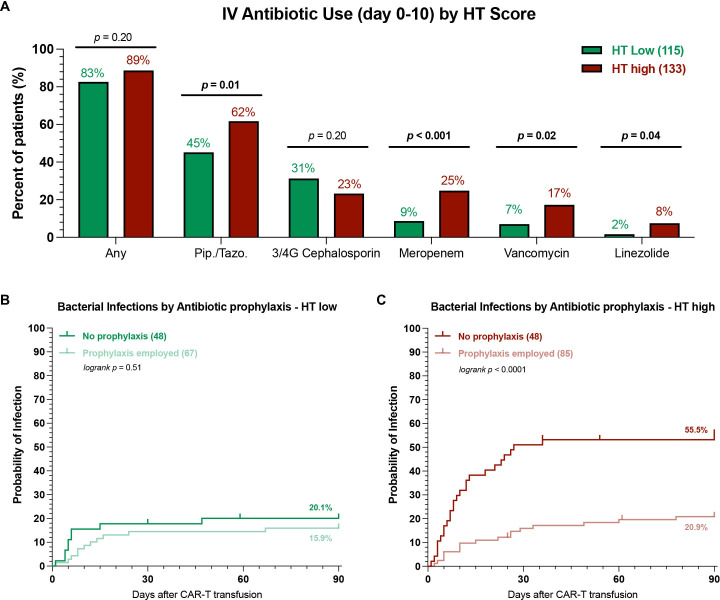
In a multivariate analysis adjusted for other baseline features, the HT score identified patients at high risk for severe infections (adjusted HR 6.4, 95% CI 3.1 to 13.1). HT patients more frequently developed severe infections (40% vs 8%, p<0.0001)-particularly severe bacterial infections (27% vs 0.9%, p<0.0001). Additionally, multivariate analysis of post-CAR-T factors revealed that infection risk was increased by prolonged neutropenia (≥14 days) and corticosteroid use (≥9 days), and decreased with fluoroquinolone prophylaxis. Antibacterial prophylaxis significantly reduced the likelihood of severe bacterial infections in HT (16% vs 46%, p<0.001), but not HT patients (0% vs 2%, p=n.s.). Collectively, HT patients experienced worse median progression-free (3.4 vs 12.6 months) and overall survival (9.1 months vs not-reached), and were hospitalized longer (median 20 vs 16 days). Severe infections represented the most common cause of non-relapse mortality after CAR-T and were associated with poor survival outcomes. A trend toward increased non-relapse mortality in HT patients was observed (8.0% vs 3.7%, p=0.09).
These data demonstrate the utility of the HT score to risk-stratify patients for infectious complications and poor survival outcomes to CD19 CAR-T. High-risk patients likely benefit from anti-infective prophylaxis and should be closely monitored for potential infections and relapse.
CD19 导向嵌合抗原受体 T 细胞疗法(CAR-T)代表了一种越来越多 B 细胞恶性肿瘤的有前途的治疗方法。然而,长期的细胞减少症和感染极大地增加了 CAR-T 的毒性负担。最近开发的 CAR-HEMATOTOX(HT)评分由五个预淋巴细胞减少变量组成(例如,绝对中性粒细胞计数、血小板计数、血红蛋白、C 反应蛋白、铁蛋白),能够对血液毒性进行风险分层。
在这项多中心回顾性分析中,我们对 248 例接受标准护理 CD19 CAR-T 治疗复发/难治性大 B 细胞淋巴瘤的患者进行了早期感染事件(0-90 天)和临床结局的特征描述。这包括一个推导队列(队列 A,179 例患者)和第二个独立验证队列(队列 B,69 例患者)。计算了所有等级、等级≥3 和特定感染亚型的累积发生率曲线。通过 Kaplan-Meier 估计研究临床结局。
在调整其他基线特征的多变量分析中,HT 评分确定了发生严重感染风险高的患者(调整后的 HR 6.4,95%CI 3.1 至 13.1)。HT 患者更频繁地发生严重感染(40%比 8%,p<0.0001),特别是严重细菌感染(27%比 0.9%,p<0.0001)。此外,CAR-T 后因素的多变量分析表明,感染风险增加与中性粒细胞减少(≥14 天)和皮质类固醇使用(≥9 天)有关,与氟喹诺酮类药物预防有关。抗菌预防显著降低了 HT 中严重细菌感染的可能性(16%比 46%,p<0.001),但对 HT 患者没有影响(0%比 2%,p=n.s.)。总体而言,HT 患者的中位无进展生存(3.4 个月比 12.6 个月)和总生存(9.1 个月比未达到)更差,住院时间更长(中位 20 天比 16 天)。严重感染是 CAR-T 后非复发死亡的最常见原因,与不良生存结局相关。在 HT 患者中观察到非复发死亡率增加的趋势(8.0%比 3.7%,p=0.09)。
这些数据表明,HT 评分可用于对接受 CD19 CAR-T 的患者进行感染并发症和不良生存结局的风险分层。高危患者可能受益于抗感染预防措施,应密切监测潜在感染和复发。