Université de Lorraine, Inserm, Centre d'Investigations Cliniques- Plurithématique 14-33, and Inserm U1116, CHRU, F-CRIN INI-CRCT (Cardiovascular and Renal Clinical Trialists), Nancy, France (N.G., K.D., J.P.F., A.P., A.-C.H., P.R., F.Z.).
National Heart, Lung, and Blood Institute's and Boston University's Framingham Heart Study, Framingham, MA (D.L., J.H., S.-J.H).
Circ Heart Fail. 2023 May;16(5):e009694. doi: 10.1161/CIRCHEARTFAILURE.122.009694. Epub 2023 May 16.
We sought to identify protein biomarkers of new-onset heart failure (HF) in 3 independent cohorts (HOMAGE cohort [Heart Omics and Ageing], ARIC study [Atherosclerosis Risk in Communities], and FHS [Framingham Heart Study]) and assess if and to what extent they improve HF risk prediction compared to clinical risk factors alone.
A nested case-control design was used with cases (incident HF) and controls (without HF) matched on age and sex within each cohort. Plasma concentrations of 276 proteins were measured at baseline in ARIC (250 cases/250 controls), FHS (191/191), and HOMAGE cohort (562/871).
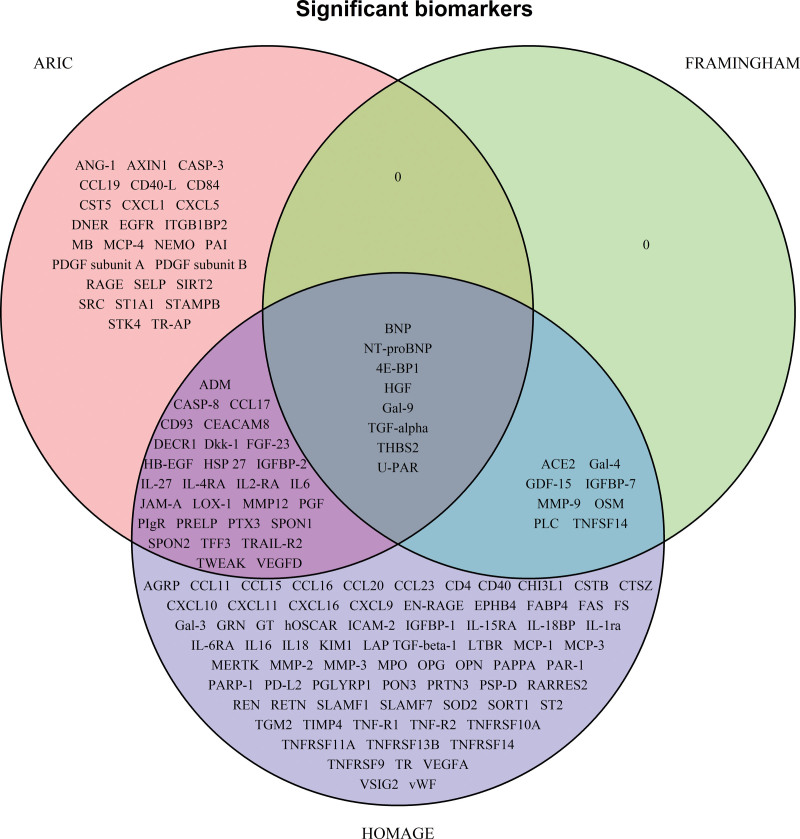
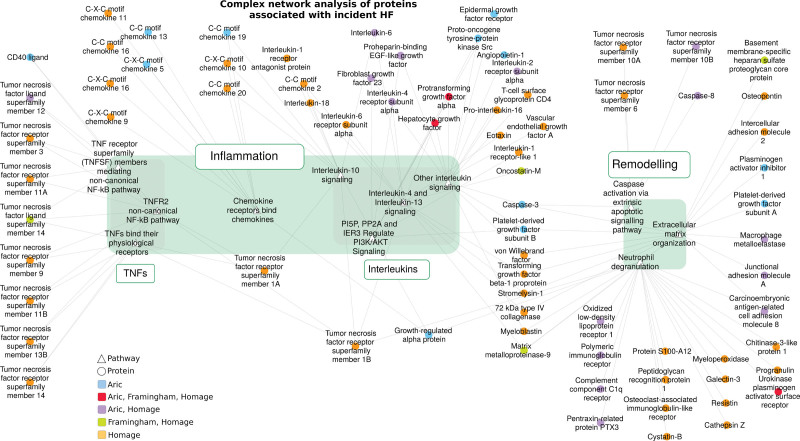
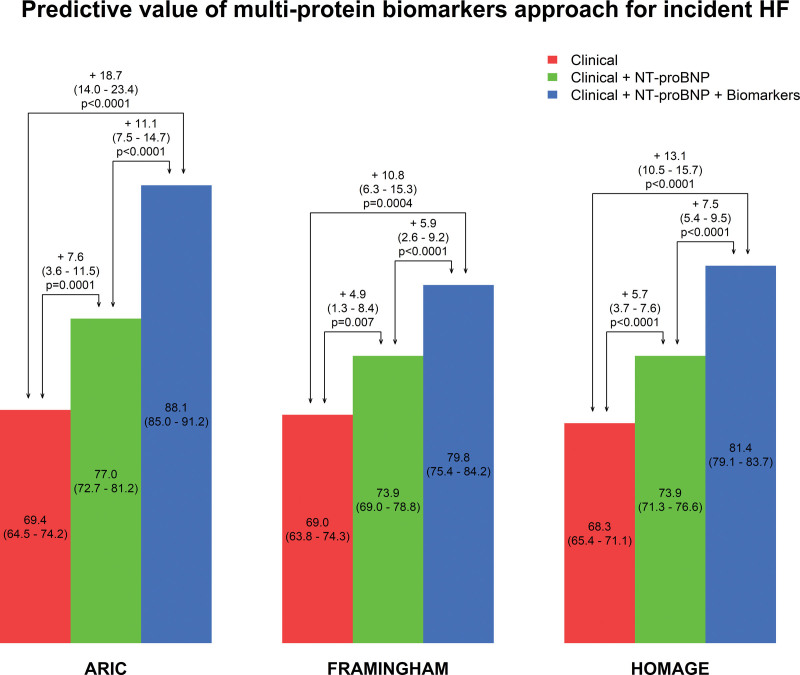
In single protein analysis, after adjusting for matching variables and clinical risk factors (and correcting for multiple testing), 62 proteins were associated with incident HF in ARIC, 16 in FHS, and 116 in HOMAGE cohort. Proteins associated with incident HF in all cohorts were BNP (brain natriuretic peptide), NT-proBNP (N-terminal pro-B-type natriuretic peptide), eukaryotic translation initiation factor 4E-BP1 (4E-binding protein 1), hepatocyte growth factor (HGF), Gal-9 (galectin-9), TGF-alpha (transforming growth factor alpha), THBS2 (thrombospondin-2), and U-PAR (urokinase plasminogen activator surface receptor). The increment in -index for incident HF based on a multiprotein biomarker approach, in addition to clinical risk factors and NT-proBNP, was 11.1% (7.5%-14.7%) in ARIC, 5.9% (2.6%-9.2%) in FHS, and 7.5% (5.4%-9.5%) in HOMAGE cohort, all <0.001), each of which was a larger increase than that for NT-proBNP on top of clinical risk factors. Complex network analysis revealed a number of overrepresented pathways related to inflammation (eg, tumor necrosis factor and interleukin) and remodeling (eg, extracellular matrix and apoptosis).
A multiprotein biomarker approach improves prediction of incident HF when added to natriuretic peptides and clinical risk factors.
我们旨在通过三个独立队列(HOMAGE 队列[心脏组学和衰老]、ARIC 研究[社区动脉粥样硬化风险]和 FHS[弗雷明汉心脏研究])识别新发生心力衰竭(HF)的蛋白生物标志物,并评估其是否以及在何种程度上优于临床危险因素单独预测 HF 风险。
采用巢式病例对照设计,在每个队列中根据年龄和性别对病例(新发 HF)和对照(无 HF)进行匹配。在 ARIC(250 例/250 例对照)、FHS(191/191)和 HOMAGE 队列(562/871)中,在基线时测量了 276 种蛋白质的血浆浓度。
在单蛋白分析中,在调整匹配变量和临床危险因素后(并校正了多重检验),ARIC 中有 62 种蛋白与新发 HF 相关,FHS 中有 16 种蛋白与新发 HF 相关,HOMAGE 队列中有 116 种蛋白与新发 HF 相关。与所有队列中发生 HF 相关的蛋白有脑钠肽(BNP)、氨基末端 B 型利钠肽前体(NT-proBNP)、真核翻译起始因子 4E 结合蛋白 1(4E 结合蛋白 1)、肝细胞生长因子(HGF)、Gal-9(半乳糖凝集素-9)、转化生长因子-α(转化生长因子-α)、THBS2(血栓素-2)和 U-PAR(尿激酶纤溶酶原激活物表面受体)。基于多蛋白生物标志物方法,除临床危险因素和 NT-proBNP 外,新发 HF 的-指数增加了 11.1%(7.5%-14.7%),在 FHS 中增加了 5.9%(2.6%-9.2%),在 HOMAGE 队列中增加了 7.5%(5.4%-9.5%),均<0.001),每个队列中的增加均大于 NT-proBNP 与临床危险因素相加的增加。复杂网络分析显示,许多与炎症(如肿瘤坏死因子和白细胞介素)和重塑(如细胞外基质和细胞凋亡)相关的代表性通路过度表达。
当多蛋白生物标志物方法与利钠肽和临床危险因素联合使用时,可以提高新发 HF 的预测准确性。