Chesapeake Urology Research Associates, Baltimore, MD, USA.
Icahn School of Medicine at Mt. Sinai, New York City, NY, USA.
Prostate Cancer Prostatic Dis. 2023 Sep;26(3):596-601. doi: 10.1038/s41391-023-00675-1. Epub 2023 May 16.
Patient outcomes were assessed based on a pre-biopsy ExoDx Prostate (EPI) score at 2.5 years of the 5-year follow-up of ongoing prostate biopsy Decision Impact Trial of the ExoDx Prostate (IntelliScore).
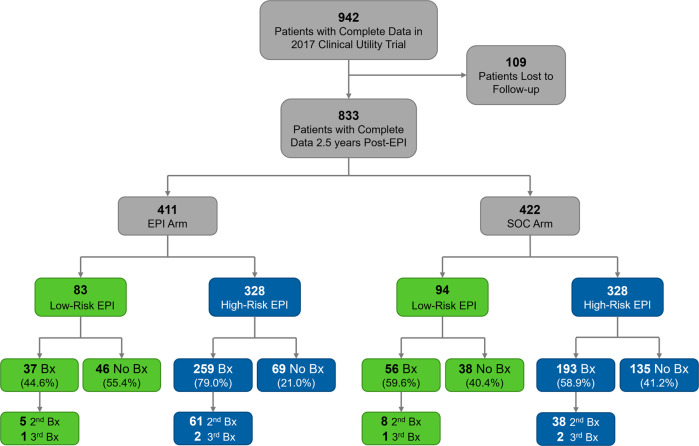
Prospective, blinded, randomized, multisite clinical utility study was conducted from June 2017 to May 2018 (NCT03235687). Urine samples were collected from 1049 men (≥50 years old) with a PSA 2-10 ng/mL being considered for a prostate biopsy. Patients were randomized to EPI vs. standard of care (SOC). All had an EPI test, but only EPI arm received results during biopsy decision process. Clinical outcomes, time to biopsy and pathology were assessed among low (<15.6) or high (≥15.6) EPI scores.
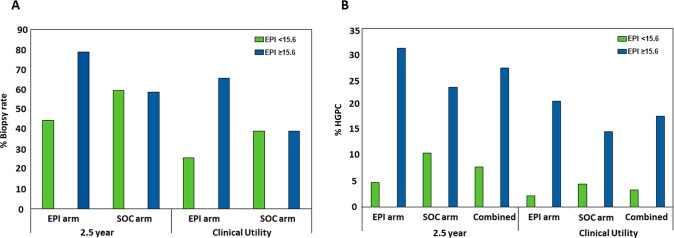
At 2.5 years, 833 patients had follow-up data. In the EPI arm, biopsy rates remained lower for low-risk EPI scores than high-risk EPI scores (44.6% vs 79.0%, p < 0.001), whereas biopsy rates were identical in SOC arm regardless of EPI score (59.6% vs 58.8%, p = 0.99). Also in the EPI arm, the average time from EPI testing to first biopsy was longer for low-risk EPI scores compared to high-risk EPI scores (216 vs. 69 days; p < 0.001). Similarly, the time to first biopsy was longer with EPI low-risk scores in EPI arm compared to EPI low-risk scores in SOC arm (216 vs 80 days; p < 0.001). At 2.5 years, patients with low-risk EPI scores from both arms had less HGPC than high-risk EPI score patients (7.9% vs 26.8%, p < 0.001) and the EPI arm found 21.8% more HGPC than the SOC arm.
This follow-up analysis captures subsequent biopsy outcomes and demonstrates that men receiving EPI low-risk scores (<15.6) significantly defer the time to first biopsy and remain at a very low pathologic risk by 2.5-years after the initial study. The EPI test risk stratification identified low-risk patients that were not found with the SOC.
基于正在进行的前列腺活检决策影响试验的 ExoDx 前列腺(IntelliScore) 5 年随访中 2 年半的活检前 ExoDx 前列腺(EPI)评分,评估患者的预后。
这是一项前瞻性、盲法、随机、多中心临床效用研究,于 2017 年 6 月至 2018 年 5 月进行(NCT03235687)。从年龄≥50 岁且前列腺特异性抗原(PSA)为 2-10ng/ml 并考虑进行前列腺活检的 1049 名男性中采集尿样。患者被随机分配到 EPI 组或标准护理(SOC)组。所有患者均进行了 EPI 检测,但仅 EPI 组在活检决策过程中获得了结果。根据 EPI 评分的高低(<15.6 或≥15.6)评估低危(<15.6)和高危(≥15.6)EPI 评分患者的临床结局、活检时间和病理情况。
2.5 年后,833 名患者有随访数据。在 EPI 组中,低危 EPI 评分的活检率仍低于高危 EPI 评分(44.6% vs. 79.0%,p<0.001),而 SOC 组中 EPI 评分对活检率没有影响(59.6% vs. 58.8%,p=0.99)。同样在 EPI 组中,与高危 EPI 评分相比,低危 EPI 评分的首次活检平均时间更长(216 天 vs. 69 天;p<0.001)。同样,EPI 低危评分患者的首次活检时间在 EPI 组中也长于 SOC 组(216 天 vs. 80 天;p<0.001)。2.5 年后,来自两组的低危 EPI 评分患者的 HGPC 发生率低于高危 EPI 评分患者(7.9% vs. 26.8%,p<0.001),且 EPI 组比 SOC 组发现 21.8%更多的 HGPC。
本随访分析捕获了随后的活检结果,并表明接受 EPI 低危评分(<15.6)的男性首次活检时间显著延迟,并且在最初研究后的 2.5 年内仍处于极低的病理风险。EPI 测试风险分层确定了 SOC 未发现的低危患者。