Wu Juei-Seng, Hong Tzu-Chun, Wu Hung-Tsung, Lin Yih-Jyh, Chang Ting-Tsung, Wang Chung-Teng, Liu Wen-Chun, Hsieh Ming-Tsung, Wu I-Chin, Chen Po-Jun, Chen Chiung-Yu, Lin Sheng-Hsiang, Chuang Chiao-Hsiung, Han Meng-Zhi, Chen Huang-Pin, Tsai Hong-Ming, Kuo Hsin-Yu
Department of Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan.
Department of Surgery, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan.
J Gastrointest Oncol. 2023 Apr 29;14(2):849-862. doi: 10.21037/jgo-22-858. Epub 2023 Apr 10.
The presence of vascular invasion is associated with poor survival in advanced hepatocellular carcinoma (HCC). We compared the effectiveness of hepatic arterial infusion chemotherapy (HAIC) and immune checkpoint inhibitors (ICIs), alone or in combination, in patients with advanced HCC.
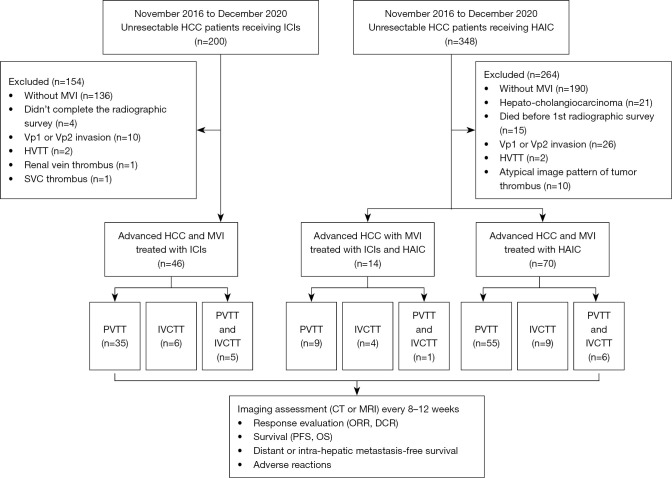
We retrospectively reviewed medical records of adult patients with unresectable HCC and macrovascular invasion (MVI) who were treated with HAIC or ICIs alone or in combination at a single centre in Taiwan. Overall tumour response, vascular thrombi response, overall survival (OS) and progression-free survival (PFS) in 130 patients were analysed.
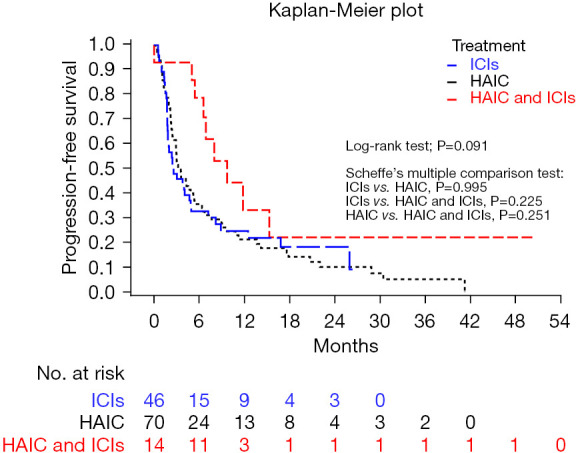
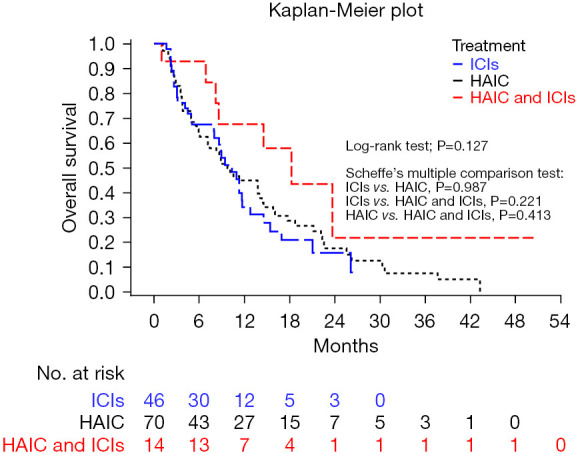
The treatment group showed no significant effect on the overall tumour response [objective response rate (ORR), 22.86% for HAIC, 26.09% for ICI, 50.00% for HAIC+ICI; P=0.111], but showed a significant effect on vessel response (objective response rate of tumour thrombi (ORRT), 38.57% for HAIC, 45.65% for ICI, 78.57% for HAIC+ICI; P=0.023). Post-hoc comparisons followed by Bonferroni correction revealed that vessel ORRT was significantly different between the HAIC+ICI and HAIC groups (P=0.014). A significant effect of treatment group on portal vein tumour thrombus (PVTT) was also detected (ORRT, 40.00% for HAIC, 50.00% for ICI, 90.00% for HAIC; P=0.013), with significant difference between the HAIC+ICI and HAIC groups (P=0.005). Patients treated with HAIC, ICI, and HAIC+ICI respectively had 12-month OS rates of 44.9%, 31.4%, and 67.5% (P=0.127) and 12-month PFS rates of 21.2%, 24.6%, and 33.2% (P=0.091). In multivariate analysis of PFS, HAIC+ICI was associated with reduced risk of progression or death compared with HAIC alone (adjusted hazard ratio: 0.46; 95% confidence interval: 0.23-0.94; P=0.032).
HAIC combined with ICIs had a superior response of PVTT compared to HAIC alone, and was associated with reduced risk of progression or death. Future studies are needed to address the survival benefit of the combination therapy in advanced HCC with MVI.
血管侵犯的存在与晚期肝细胞癌(HCC)的不良生存相关。我们比较了肝动脉灌注化疗(HAIC)和免疫检查点抑制剂(ICI)单独或联合应用于晚期HCC患者的疗效。
我们回顾性分析了台湾某单一中心接受HAIC或ICI单独或联合治疗的不可切除HCC和大血管侵犯(MVI)成年患者的病历。分析了130例患者的总体肿瘤反应、血管血栓反应、总生存期(OS)和无进展生存期(PFS)。
治疗组对总体肿瘤反应无显著影响[客观缓解率(ORR),HAIC为22.86%,ICI为26.09%,HAIC+ICI为50.00%;P=0.111],但对血管反应有显著影响(肿瘤血栓客观缓解率(ORRT),HAIC为38.57%,ICI为45.65%,HAIC+ICI为78.57%;P=0.023)。采用Bonferroni校正后的事后比较显示,HAIC+ICI组与HAIC组之间的血管ORRT有显著差异(P=0.014)。还检测到治疗组对门静脉肿瘤血栓(PVTT)有显著影响(ORRT,HAIC为40.00%,ICI为50.00%,HAIC+ICI为90.00%;P=0.013),HAIC+ICI组与HAIC组之间有显著差异(P=0.005)。接受HAIC、ICI和HAIC+ICI治疗的患者12个月OS率分别为44.9%、31.4%和67.5%(P=0.127),12个月PFS率分别为21.2%、24.6%和33.2%(P=0.091)。在PFS的多因素分析中,与单独使用HAIC相比,HAIC+ICI与进展或死亡风险降低相关(调整后风险比:0.46;95%置信区间:0.23-0.94;P=0.032)。
与单独使用HAIC相比,HAIC联合ICI对PVTT的反应更佳,且与进展或死亡风险降低相关。未来需要开展研究以探讨联合治疗对伴有MVI的晚期HCC患者的生存获益。