Division of Hospital Medicine, Michigan Medicine, University of Michigan, Ann Arbor, Michigan, USA
Partners In Health, Boston, Massachusetts, USA.
BMJ Open. 2023 May 18;13(5):e067343. doi: 10.1136/bmjopen-2022-067343.
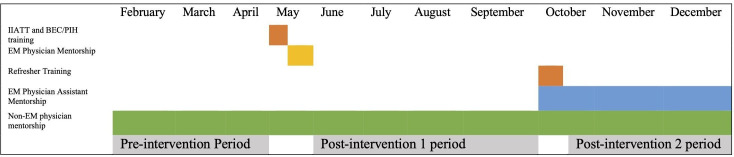
In Liberia, emergency care is still in its early development. In 2019, two emergency care and triage education sessions were done at J. J. Dossen Hospital in Southeastern Liberia. The observational study objectives evaluated key process outcomes before and after the educational interventions.
Emergency department paper records from 1 February 2019 to 31 December 2019 were retrospectively reviewed. Simple descriptive statistics were used to describe patient demographics and χ analyses were used to test for significance. ORs were calculated for key predetermined process measures.
There were 8222 patient visits recorded that were included in our analysis. Patients in the post-intervention 1 group had higher odds of having a documented full set of vital signs compared with the baseline group (16% vs 3.5%, OR: 5.4 (95% CI: 4.3 to 6.7)). After triage implementation, patients who were triaged were 16 times more likely to have a full set of vitals compared with those who were not triaged. Similarly, compared with the baseline group, patients in the post-intervention 1 group had higher odds of having a glucose documented if they presented with altered mental status or a neurologic complaint (37% vs 30%, OR: 1.7 (95% CI: 1.3 to 2.2)), documented antibiotic administration if they had a presumed bacterial infection (87% vs 35%, OR: 12.8 (95% CI: 8.8 to 17.1)), documented malaria test if presenting with fever (76% vs 61%, OR: 2.05 (95% CI: 1.37 to 3.08)) or documented repeat set of vitals if presenting with shock (25% vs 6.6%, OR: 8.85 (95% CI: 1.67 to 14.06)). There was no significant difference in the above process outcomes between the education interventions.
This study showed improvement in most process measures between the baseline and post-intervention 1 groups, benefits that persisted post-intervention 2, thus supporting the importance of short-course education interventions to durably improve facility-based care.
在利比里亚,紧急护理仍处于早期发展阶段。2019 年,在利比里亚东南部的 JJ Dossen 医院进行了两次紧急护理和分诊教育课程。本观察性研究的目的是评估教育干预前后的关键流程结果。
回顾性分析 2019 年 2 月 1 日至 12 月 31 日期间的急诊病历。采用简单描述性统计方法描述患者人口统计学特征,并采用 χ 检验进行显著性检验。对于关键预定流程指标,计算了比值比(OR)。
共记录了 8222 例患者就诊,纳入本分析。与基线组相比,干预 1 组的患者更有可能记录完整的一套生命体征(16%比 3.5%,OR:5.4(95%CI:4.3 至 6.7))。分诊实施后,与未分诊的患者相比,分诊患者记录完整生命体征的可能性高出 16 倍。同样,与基线组相比,在干预 1 组中,出现精神状态改变或神经系统症状的患者记录血糖的可能性更高(37%比 30%,OR:1.7(95%CI:1.3 至 2.2)),有疑似细菌感染的患者记录抗生素使用情况的可能性更高(87%比 35%,OR:12.8(95%CI:8.8 至 17.1)),出现发热的患者记录疟疾检查的可能性更高(76%比 61%,OR:2.05(95%CI:1.37 至 3.08)),出现休克的患者记录重复生命体征的可能性更高(25%比 6.6%,OR:8.85(95%CI:1.67 至 14.06))。两次教育干预之间,上述流程结果没有显著差异。
本研究显示,在基线组和干预 1 组之间,大多数流程指标均有所改善,且在干预 2 后仍持续获益,因此支持短期课程教育干预对持久改善医疗机构护理的重要性。