Holst Jenelle A, Perman Sarah M, Capp Roberta, Haukoos Jason S, Ginde Adit A
University of Colorado School of Medicine, Department of Emergency Medicine, Aurora, Colorado; Denver Health Medical Center, Department of Emergency Medicine, Denver, Colorado.
University of Colorado School of Medicine, Department of Emergency Medicine, Aurora, Colorado.
West J Emerg Med. 2016 May;17(3):315-23. doi: 10.5811/westjem.2016.2.29327. Epub 2016 May 2.
Accurate field triage of critically injured patients to trauma centers is vital for improving survival. We sought to estimate the national degree of undertriage of trauma patients who die in emergency departments (EDs) by evaluating the frequency and characteristics associated with triage to non-trauma centers.
This was a retrospective cross-sectional analysis of adult ED trauma deaths in the 2010 National Emergency Department Sample (NEDS). The primary outcome was appropriate triage to a trauma center (Level I, II or III) or undertriage to a non-trauma center. We subsequently focused on urban areas given improved access to trauma centers. We evaluated the associations of patient demographics, hospital region and mechanism of injury with triage to a trauma versus non-trauma center using multivariable logistic regression.
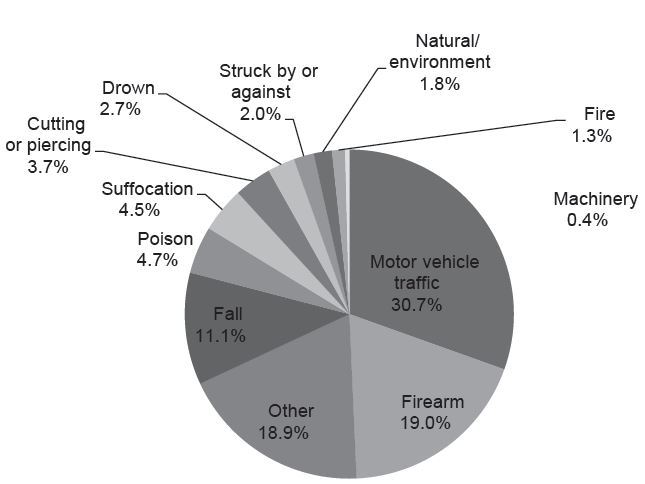
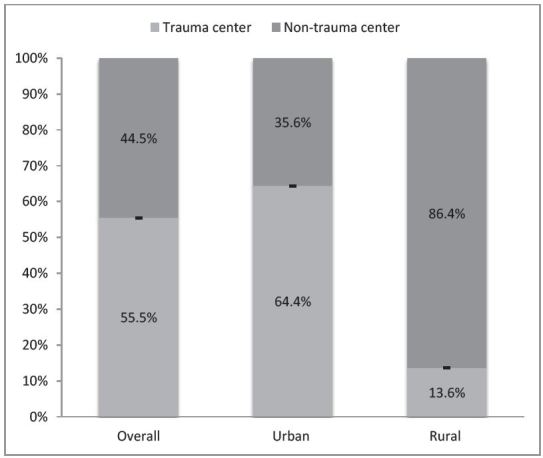
We analyzed 3,971 included visits, representing 18,464 adult ED trauma-related deaths nationally. Of all trauma deaths, nearly half (44.5%, 95% CI [43.0-46.0]) of patients were triaged to non-trauma centers. In a subgroup analysis, over a third of urban ED visits (35.6%, 95% CI [34.1-37.1]) and most rural ED visits (86.4%, 95% CI [81.5-90.1]) were triaged to non-trauma centers. In urban EDs, female patients were less likely to be triaged to trauma centers versus non-trauma centers (adjusted odds ratio [OR] 0.83, 95% CI [0.70-0.99]). Highest median household income zip codes (≥$67,000) were less likely to be triaged to trauma centers than lowest median income ($1-40,999) (OR 0.54, 95% CI [0.43-0.69]). Compared to motor vehicle trauma, firearm trauma had similar odds of being triaged to a trauma center (OR 0.90, 95% CI [0.71-1.14]); however, falls were less likely to be triaged to a trauma center (OR 0.50, 95 %CI [0.38-0.66]).
We found that nearly half of all trauma patients nationally and one-third of urban trauma patients, who died in the ED, were triaged to non-trauma centers, and thus undertriaged. Sex and other demographic disparities associated with this triage decision represent targeted opportunities to improve our trauma systems and reduce undertriage.
对重伤患者进行准确的现场分诊,将其送往创伤中心,对于提高生存率至关重要。我们试图通过评估与分诊至非创伤中心相关的频率和特征,来估计在急诊科死亡的创伤患者的全国分诊不足程度。
这是一项对2010年国家急诊科样本(NEDS)中成年急诊科创伤死亡病例的回顾性横断面分析。主要结果是是否被正确分诊至创伤中心(一级、二级或三级)或分诊不足而被送往非创伤中心。鉴于前往创伤中心的机会增加,我们随后将重点放在城市地区。我们使用多变量逻辑回归评估患者人口统计学特征、医院所在地区和损伤机制与分诊至创伤中心或非创伤中心之间的关联。
我们分析了3971例纳入的就诊病例,代表全国18464例成年急诊科创伤相关死亡病例。在所有创伤死亡病例中,近一半(44.5%,95%可信区间[43.0 - 46.0])的患者被分诊至非创伤中心。在亚组分析中,超过三分之一的城市急诊科就诊病例(35.6%,95%可信区间[34.1 - 37.1])和大多数农村急诊科就诊病例(86.4%,95%可信区间[81.5 - 90.1])被分诊至非创伤中心。在城市急诊科,女性患者被分诊至创伤中心而非非创伤中心的可能性较小(调整后的优势比[OR]为0.83,9/5%可信区间[0.70 - 0./99])。家庭收入中位数最高的邮政编码区域(≥67000美元)比分诊至创伤中心的可能性低于家庭收入中位数最低的区域(1 - 40999美元)(OR为0.54,95%可信区间[0.43 - 0.69])。与机动车创伤相比,火器创伤被分诊至创伤中心的可能性相似(OR为0.90,95%可信区间[0.71 - 1.14]);然而,跌倒被分诊至创伤中心的可能性较小(OR为0.50,95%可信区间[0.38 - 0.66])。
我们发现,在全国所有创伤患者中,近一半以及在急诊科死亡的城市创伤患者中有三分之一被分诊至非创伤中心,因此存在分诊不足的情况。与这一分诊决定相关的性别和其他人口统计学差异是改善我们的创伤系统和减少分诊不足的有针对性的机会。