Dalla Libera Alberto, Toffanin Chiara, Drecogna Martina, Galderisi Alfonso, Pillonetto Gianluigi, Cobelli Claudio
Department of Woman and Child's Health, University of Padova, 35128 Padova, Italy.
Department of Electrical, Computer and Biomedical Engineering, University of Pavia, 27100 Pavia, Italy.
APL Bioeng. 2023 May 23;7(2):026105. doi: 10.1063/5.0145446. eCollection 2023 Jun.
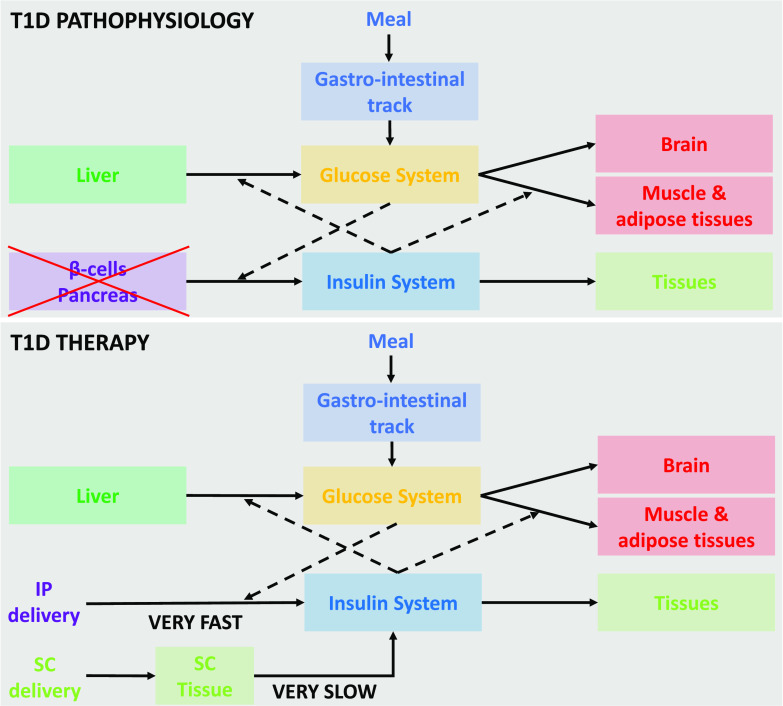
Type 1 diabetes (T1D) is a chronic autoimmune disease featured by the loss of beta cell function and the need for lifetime insulin replacement. Over the recent decade, the use of automated insulin delivery systems (AID) has shifted the paradigm of treatment: the availability of continuous subcutaneous (SC) glucose sensors to guide SC insulin delivery through a control algorithm has allowed, for the first time, to reduce the daily burden of the disease as well as to abate the risk for hypoglycemia. AID use is still limited by individual acceptance, local availability, coverage, and expertise. A major drawback of SC insulin delivery is the need for meal announcement and the peripheral hyperinsulinemia that, over time, contributes to macrovascular complications. Inpatient trials using intraperitoneal (IP) insulin pumps have demonstrated that glycemic control can be improved without meal announcement due to the faster insulin delivery through the peritoneal space. This calls for novel control algorithms able to account for the specificities of IP insulin kinetics. Recently, our group described a two-compartment model of IP insulin kinetics demonstrating that the peritoneal space acts as a virtual compartment and IP insulin delivery is virtually intraportal (intrahepatic), thus closely mimicking the physiology of insulin secretion. The FDA-accepted T1D simulator for SC insulin delivery and sensing has been updated for IP insulin delivery and sensing. Herein, we design and validate-a time-varying proportional integrative derivative controller to guide IP insulin delivery in a fully closed-loop mode without meal announcement.
1型糖尿病(T1D)是一种慢性自身免疫性疾病,其特征是β细胞功能丧失,需要终身进行胰岛素替代治疗。在过去十年中,自动胰岛素输送系统(AID)的使用改变了治疗模式:连续皮下(SC)葡萄糖传感器的可用性通过控制算法来指导皮下胰岛素输送,首次使得减轻疾病的日常负担以及降低低血糖风险成为可能。AID的使用仍然受到个体接受度、当地可用性、覆盖范围和专业知识的限制。皮下胰岛素输送的一个主要缺点是需要进行进餐告知以及外周高胰岛素血症,随着时间的推移,这会导致大血管并发症。使用腹腔内(IP)胰岛素泵的住院试验表明,由于胰岛素通过腹膜腔的输送速度更快,无需进餐告知即可改善血糖控制。这就需要能够考虑到腹腔内胰岛素动力学特性的新型控制算法。最近,我们团队描述了一种腹腔内胰岛素动力学的双室模型,表明腹膜腔起到了一个虚拟腔室的作用,腹腔内胰岛素输送实际上是门静脉内(肝内)输送,因此紧密模拟了胰岛素分泌的生理过程。用于皮下胰岛素输送和传感的FDA认可的T1D模拟器已针对腹腔内胰岛素输送和传感进行了更新。在此,我们设计并验证了一种时变比例积分微分控制器,以在无需进餐告知的完全闭环模式下指导腹腔内胰岛素输送。