Southeastern National Tuberculosis Center, Division of Infectious Diseases and Global Medicine, Department of Medicine in the College of Medicine, University of Florida, Gainesville, Florida, USA.
Division of Infectious Diseases, Department of Medicine, Vanderbilt University Medical Center, Nashville, Tennessee, USA.
Clin Infect Dis. 2023 Oct 5;77(7):1053-1062. doi: 10.1093/cid/ciad312.
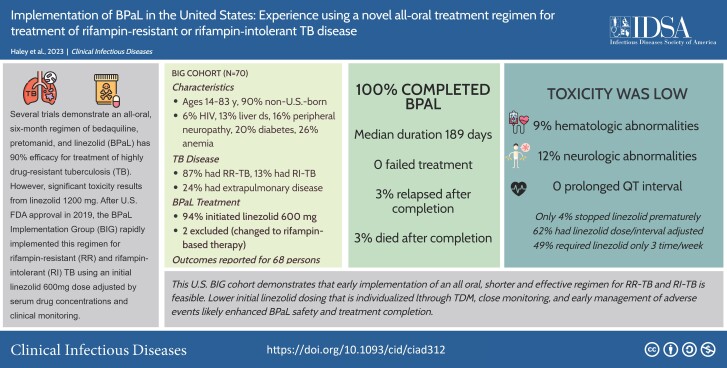
Rifampin-resistant tuberculosis is a leading cause of morbidity worldwide; only one-third of persons start treatment, and outcomes are often inadequate. Several trials demonstrate 90% efficacy using an all-oral, 6-month regimen of bedaquiline, pretomanid, and linezolid (BPaL), but significant toxicity occurred using 1200-mg linezolid. After US Food and Drug Administration approval in 2019, some US clinicians rapidly implemented BPaL using an initial 600-mg linezolid dose adjusted by serum drug concentrations and clinical monitoring.
Data from US patients treated with BPaL between 14 October 2019 and 30 April 2022 were compiled and analyzed by the BPaL Implementation Group (BIG), including baseline examination and laboratory, electrocardiographic, and clinical monitoring throughout treatment and follow-up. Linezolid dosing and clinical management was provider driven, and most patients had linezolid adjusted by therapeutic drug monitoring.
Of 70 patients starting BPaL, 2 changed to rifampin-based therapy, 68 (97.1%) completed BPaL, and 2 of the 68 (2.9%) experienced relapse after completion. Using an initial 600-mg linezolid dose daily adjusted by therapeutic drug monitoring and careful clinical and laboratory monitoring for adverse effects, supportive care, and expert consultation throughout BPaL treatment, 3 patients (4.4%) with hematologic toxicity and 4 (5.9%) with neurotoxicity required a change in linezolid dose or frequency. The median BPaL duration was 6 months.
BPaL has transformed treatment for rifampin-resistant or intolerant tuberculosis. In this cohort, effective treatment required less than half the duration recommended in 2019 US guidelines for drug-resistant tuberculosis. Use of individualized linezolid dosing and monitoring likely enhanced safety and treatment completion. The BIG cohort demonstrates that early implementation of new tuberculosis treatments in the United States is feasible.
利福平耐药结核病是全球发病率的主要原因;只有三分之一的人开始治疗,而且结果往往不理想。几项试验表明,使用贝达喹啉、普托马尼德和利奈唑胺(BPaL)的全口服、6 个月疗程的疗效为 90%,但使用 1200 毫克利奈唑胺时会出现显著毒性。2019 年美国食品和药物管理局批准后,一些美国临床医生迅速使用 BPaL,初始剂量为 600 毫克利奈唑胺,根据血清药物浓度和临床监测进行调整。
BPaL 实施小组(BIG)汇编并分析了 2019 年 10 月 14 日至 2022 年 4 月 30 日期间接受 BPaL 治疗的美国患者的数据,包括基线检查和实验室、心电图和整个治疗和随访期间的临床监测。利奈唑胺的剂量和临床管理由提供者驱动,大多数患者接受利奈唑胺的治疗药物监测调整。
70 名开始使用 BPaL 的患者中,有 2 名改为基于利福平的治疗,68 名(97.1%)完成了 BPaL,68 名中的 2 名(2.9%)在完成后复发。使用初始 600 毫克利奈唑胺剂量,每天根据治疗药物监测进行调整,并在整个 BPaL 治疗期间仔细进行临床和实验室监测以预防不良反应、提供支持性护理和咨询专家,3 名(4.4%)有血液毒性和 4 名(5.9%)有神经毒性的患者需要调整利奈唑胺的剂量或频率。BPaL 的中位持续时间为 6 个月。
BPaL 改变了耐利福平或不耐受利福平结核病的治疗方法。在本队列中,有效的治疗所需时间不到 2019 年美国耐多药结核病指南建议的一半。使用个体化利奈唑胺剂量和监测可能提高了安全性和治疗完成率。BIG 队列表明,在美国早期实施新的结核病治疗是可行的。