Department of Orthopaedics, Shanghai Sixth People's Hospital, Shanghai, China.
Institute of Clinical Research, National Center for Orthopaedics, Shanghai Sixth People's Hospital, Shanghai, China.
Ann Rheum Dis. 2023 Sep;82(9):1218-1226. doi: 10.1136/ard-2023-223845. Epub 2023 May 31.
Obesity is a risk factor for knee osteoarthritis (KOA) development and progression. Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are indicated for type 2 diabetes mellitus (T2DM) and obesity. However, whether KOA patients can benefit from GLP-1RA therapies has not been sufficiently investigated, especially in the long term.
The Shanghai Osteoarthritis Cohort study is a prospective, observational, multicentre study of >40 000 adults with clinically diagnosed osteoarthritis aged >45 years in Shanghai. We identified all KOA participants with comorbid T2DM enrolled from 1 January 2011 to 1 January 2017. Primary outcome was incidence of knee surgery after enrolment. Secondary outcomes included pain-relieving medication use, number of intra-articular therapies, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and medial femorotibial joint cartilage thickness. To evaluate the effects of GLP-1RA, we performed before-and-after comparison and comparison with participants who had no GLP-1RA exposure.
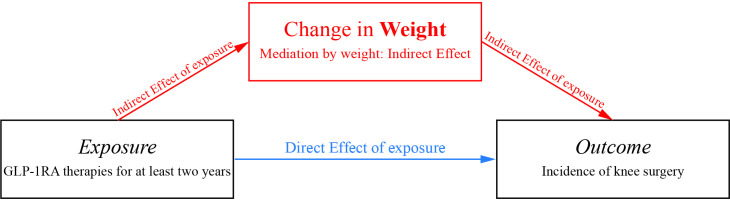
For an intergroup comparison (non-GLP-1RA vs GLP-1RA), more weight loss (adjusted mean difference in weight change from baseline -7.29 kg (95% CI -8.07 to -6.50 kg), p<0.001) and lower incidence of knee surgery (93/1574 (5.9%) vs 4/233 (1.7%), adjusted p=0.014) were observed in the GLP-1RA group. Statistically significant differences in mean change from baseline for the WOMAC total and pain subscale scores were observed (adjusted mean difference in WOMAC total score -1.46 (95% CI -2.84 to -0.08), p=0.038; adjusted mean difference in WOMAC pain subscore -3.37 (95% CI -5.79 to -0.94), p=0.007). Cartilage-loss velocity of the medial femorotibial joint was significantly lower in the GLP-1RA group postadjustment for baseline characteristics (adjusted mean difference -0.02 mm (95% CI -0.03 to -0.002 mm), p=0.004). For the before-and-after comparison within the GLP-1RA group, we observed a significant decrease of symptom-relieving medication consumption and cartilage loss velocity of medial femorotibial joint (after-treatment vs before-treatment: -0.03±0.05 vs -0.05±0.07 mm/year, p<0.001). The association between GLP-1RA exposure and decreased incidence of knee surgery was mediated by weight reduction (mediation proportion: 32.1%), instead of glycaemic control (too small to calculate).
With sufficient treatment duration, GLP-1RA therapies might be disease-modifying for KOA patients with comorbid T2DM, possibly mediated by weight loss. Further investigation is needed to elucidate effects of GLP-1RA on disease process, joint structure and patient-reported outcomes of osteoarthritis.
肥胖是膝关节骨关节炎(KOA)发展和进展的一个危险因素。胰高血糖素样肽-1 受体激动剂(GLP-1RAs)适用于 2 型糖尿病(T2DM)和肥胖症。然而,KOA 患者是否能从 GLP-1RA 治疗中获益尚未得到充分研究,尤其是在长期方面。
上海骨关节炎队列研究是一项针对>40000 名年龄>45 岁的有临床诊断为骨关节炎的成年人的前瞻性、观察性、多中心研究。我们从 2011 年 1 月 1 日至 2017 年 1 月 1 日,确定了所有患有 T2DM 合并 KOA 的 KOA 参与者。主要结局是登记后膝关节手术的发生率。次要结局包括缓解疼痛药物的使用、关节内治疗的次数、西部安大略省和麦克马斯特大学骨关节炎指数(WOMAC)和内侧股骨胫骨关节软骨厚度。为了评估 GLP-1RA 的作用,我们进行了前后对比,并与没有 GLP-1RA 暴露的参与者进行了对比。
对于组间比较(非 GLP-1RA 组与 GLP-1RA 组),GLP-1RA 组体重减轻更多(体重变化的调整平均差异-7.29kg(95%CI-8.07 至-6.50kg),p<0.001),膝关节手术的发生率更低(93/1574(5.9%)vs 4/233(1.7%),调整后 p=0.014)。WOMAC 总评分和疼痛子评分的平均变化从基线开始有统计学意义(WOMAC 总评分的调整平均差异-1.46(95%CI-2.84 至-0.08),p=0.038;WOMAC 疼痛子评分的调整平均差异-3.37(95%CI-5.79 至-0.94),p=0.007)。调整基线特征后,内侧股骨胫骨关节的软骨损失速度在 GLP-1RA 组中明显较低(调整平均差异-0.02mm(95%CI-0.03 至-0.002mm),p=0.004)。在 GLP-1RA 组内进行前后对比时,我们观察到缓解疼痛药物的使用量和内侧股骨胫骨关节软骨损失速度显著下降(治疗后与治疗前:-0.03±0.05 与-0.05±0.07mm/年,p<0.001)。GLP-1RA 暴露与膝关节手术发生率降低之间的关联是通过体重减轻介导的(中介比例:32.1%),而不是通过血糖控制介导的(太小而无法计算)。
在足够的治疗时间内,GLP-1RA 治疗可能对合并 T2DM 的 KOA 患者具有疾病修饰作用,可能通过体重减轻介导。需要进一步研究以阐明 GLP-1RA 对骨关节炎疾病进程、关节结构和患者报告结局的影响。