Department of Vascular Medicine, University Medical Center Utrecht, PO Box 85500, 3508 GA, Utrecht, The Netherlands.
British Heart Foundation Cardiovascular Epidemiology Unit, Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK.
Eur J Prev Cardiol. 2023 Oct 26;30(15):1705-1714. doi: 10.1093/eurjpc/zwad187.
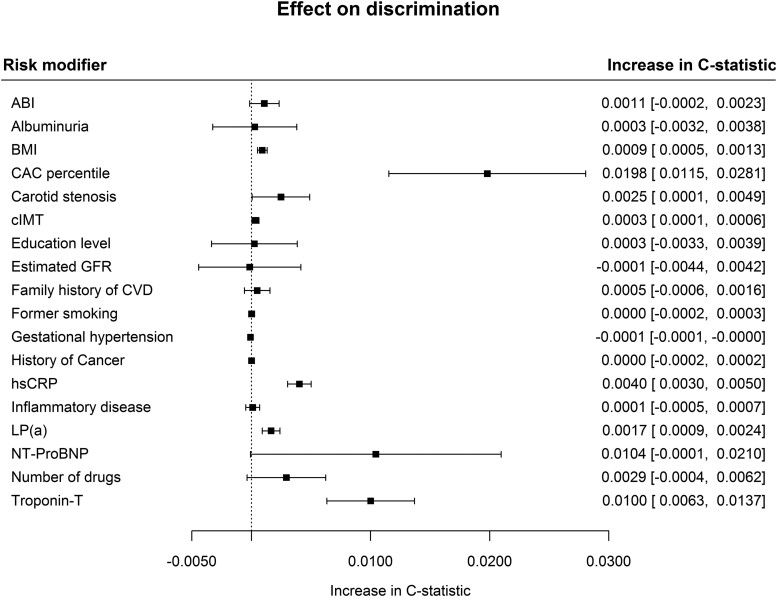
In clinical practice, factors associated with cardiovascular disease (CVD) like albuminuria, education level, or coronary artery calcium (CAC) are often known, but not incorporated in cardiovascular risk prediction models. The aims of the current study were to evaluate a methodology for the flexible addition of risk modifying characteristics on top of SCORE2 and to quantify the added value of several clinically relevant risk modifying characteristics.
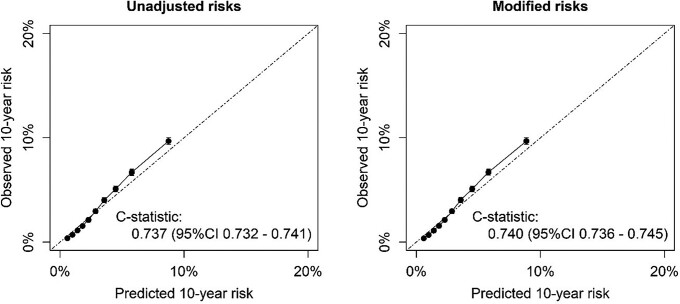
Individuals without previous CVD or DM were included from the UK Biobank; Atherosclerosis Risk in Communities (ARIC); Multi-Ethnic Study of Atherosclerosis (MESA); European Prospective Investigation into Cancer, The Netherlands (EPIC-NL); and Heinz Nixdorf Recall (HNR) studies (n = 409 757) in whom 16 166 CVD events and 19 149 non-cardiovascular deaths were observed over exactly 10.0 years of follow-up. The effect of each possible risk modifying characteristic was derived using competing risk-adjusted Fine and Gray models. The risk modifying characteristics were applied to individual predictions with a flexible method using the population prevalence and the subdistribution hazard ratio (SHR) of the relevant predictor. Risk modifying characteristics that increased discrimination most were CAC percentile with 0.0198 [95% confidence interval (CI) 0.0115; 0.0281] and hs-Troponin-T with 0.0100 (95% CI 0.0063; 0.0137). External validation was performed in the Clinical Practice Research Datalink (CPRD) cohort (UK, n = 518 015, 12 675 CVD events). Adjustment of SCORE2-predicted risks with both single and multiple risk modifiers did not negatively affect calibration and led to a modest increase in discrimination [0.740 (95% CI 0.736-0.745) vs. unimproved SCORE2 risk C-index 0.737 (95% CI 0.732-0.741)].
The current paper presents a method on how to integrate possible risk modifying characteristics that are not included in existing CVD risk models for the prediction of CVD event risk in apparently healthy people. This flexible methodology improves the accuracy of predicted risks and increases applicability of prediction models for individuals with additional risk known modifiers.
在临床实践中,与心血管疾病(CVD)相关的因素,如蛋白尿、受教育程度或冠状动脉钙(CAC),通常是已知的,但未纳入心血管风险预测模型。本研究旨在评估一种在 SCORE2 基础上灵活添加风险修饰特征的方法,并量化几种临床相关风险修饰特征的附加值。
本研究纳入了来自英国生物库(UK Biobank)、社区动脉粥样硬化风险研究(ARIC)、动脉粥样硬化多民族研究(MESA)、荷兰癌症前瞻性研究(EPIC-NL)和海因茨·尼克斯多夫回顾研究(HNR)的无既往 CVD 或 DM 的个体(n=409757),在 10.0 年的随访期间共观察到 16166 例 CVD 事件和 19149 例非心血管死亡。使用竞争风险调整的 Fine 和 Gray 模型得出每个可能的风险修饰特征的效果。使用个体预测的灵活方法,根据人群患病率和相关预测因素的亚分布危险比(SHR)应用风险修饰特征。增加最大区分度的风险修饰特征是 CAC 百分位数,为 0.0198[95%置信区间(CI)0.0115;0.0281],高敏肌钙蛋白 T 为 0.0100(95%CI 0.0063;0.0137)。在临床实践研究数据库(CPRD)队列(英国,n=518015,12675 例 CVD 事件)中进行了外部验证。使用单一和多种风险修饰物调整 SCORE2 预测风险不会对校准产生负面影响,并适度提高了区分度[0.740(95%CI 0.736-0.745)vs. 未改进的 SCORE2 风险 C 指数 0.737(95%CI 0.732-0.741)]。
本研究提出了一种方法,可以将现有 CVD 风险模型中未包含的可能风险修饰特征纳入预测无明显心血管疾病个体的 CVD 事件风险。这种灵活的方法可以提高预测风险的准确性,并增加具有已知附加风险修饰因素的个体的预测模型适用性。