Johns Hopkins Ciccarone Center for Prevention of Cardiovascular Disease, Johns Hopkins University School of Medicine, Blalock 524D1, 600 N Wolfe St, Baltimore, MD 21287, USA.
Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
Eur Heart J Cardiovasc Imaging. 2022 Apr 18;23(5):708-716. doi: 10.1093/ehjci/jeab099.
This study explored the association of coronary artery calcium (CAC) with incident cancer subtypes in the Multi-Ethnic Study of Atherosclerosis (MESA). CAC is an established predictor of cardiovascular disease (CVD), with emerging data also supporting independent predictive value for cancer. The association of CAC with risk for individual cancer subtypes is unknown.
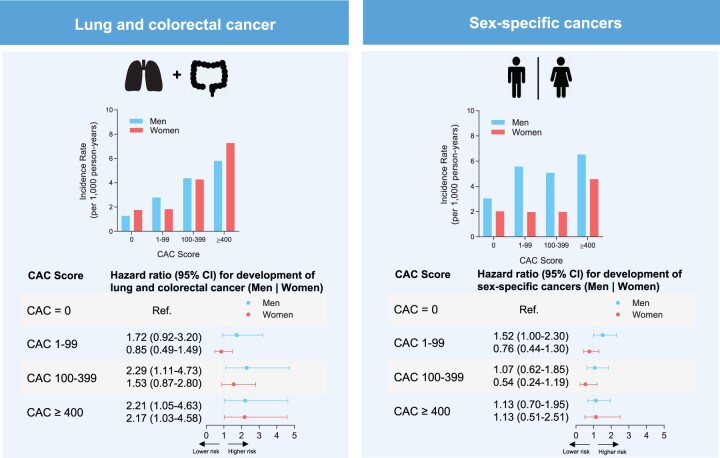
We included 6271 MESA participants, aged 45-84 and without known CVD or self-reported history of cancer. There were 777 incident cancer cases during mean follow-up of 12.9 ± 3.1 years. Lung and colorectal cancer (186 cases) were grouped based on their strong overlap with CVD risk profile; prostate (men) and ovarian, uterine, and breast cancer (women) were considered as sex-specific cancers (in total 250 cases). Incidence rates and Fine and Gray competing risks models were used to assess relative risk of cancer-specific outcomes stratified by CAC groups or Log(CAC+1). The mean age was 61.7 ± 10.2 years, 52.7% were women, and 36.5% were White. Overall, all-cause cancer incidence increased with CAC scores, with rates per 1000 person-years of 13.1 [95% confidence interval (CI): 11.7-14.7] for CAC = 0 and 35.8 (95% CI: 30.2-42.4) for CAC ≥400. Compared with CAC = 0, hazards for those with CAC ≥400 were increased for lung and colorectal cancer in men [subdistribution hazard ratio (SHR): 2.2 (95% CI: 1.1-4.7)] and women [SHR: 2.2 (95% CI: 1.0-4.6)], but not significantly for sex-specific cancers across sexes.
CAC scores were associated with cancer risk in both sexes; however, this was stronger for lung and colorectal when compared with sex-specific cancers. Our data support potential synergistic use of CAC scores in the identification of both CVD and lung and colorectal cancer risk.
本研究旨在探讨冠状动脉钙(CAC)与动脉粥样硬化多民族研究(MESA)中癌症亚型发病的相关性。CAC 是心血管疾病(CVD)的既定预测因子,越来越多的数据也支持其对癌症具有独立的预测价值。CAC 与个体癌症亚型风险的相关性尚不清楚。
我们纳入了 6271 名年龄在 45-84 岁之间、无已知 CVD 或自我报告癌症病史的 MESA 参与者。在平均 12.9±3.1 年的随访期间,共发生了 777 例癌症病例。根据与 CVD 风险特征的强烈重叠,将肺癌和结直肠癌(186 例)分为一组;前列腺癌(男性)和卵巢癌、子宫癌和乳腺癌(女性)被视为特定性别癌症(共计 250 例)。使用发病率和 Fine 和 Gray 竞争风险模型,根据 CAC 分组或 Log(CAC+1)评估癌症特异性结局的相对风险。平均年龄为 61.7±10.2 岁,52.7%为女性,36.5%为白人。总体而言,CAC 评分越高,全因癌症发病率越高,每 1000 人年的发病率分别为 CAC=0 时的 13.1[95%置信区间(CI):11.7-14.7]和 CAC≥400 时的 35.8(95%CI:30.2-42.4)。与 CAC=0 相比,CAC≥400 的男性肺癌和结直肠癌的危险度增加[亚分布危险比(SHR):2.2(95%CI:1.1-4.7)]和女性[SHR:2.2(95%CI:1.0-4.6)],但跨性别特定性别癌症的危险度无显著增加。
CAC 评分与两性的癌症风险相关;然而,与特定性别的癌症相比,这种相关性在肺癌和结直肠癌中更强。我们的数据支持 CAC 评分在识别 CVD 和肺癌及结直肠癌风险方面的潜在协同作用。