Department of Psychology and Speech-Language Pathology, Turku Brain and Mind Center, University of Turku, Turku, Finland; Department of Perioperative Services, Intensive Care and Pain Medicine, Turku University Hospital, Turku, Finland; Department of Cognitive Neuroscience and Philosophy, School of Bioscience, University of Skövde, Skövde, Sweden.
Turku PET Centre, University of Turku and Turku University Hospital, Turku, Finland.
Br J Anaesth. 2023 Aug;131(2):348-359. doi: 10.1016/j.bja.2023.04.026. Epub 2023 May 31.
Anaesthetic-induced unresponsiveness and non-rapid eye movement (NREM) sleep share common neural pathways and neurophysiological features. We hypothesised that these states bear resemblance also at the experiential level.
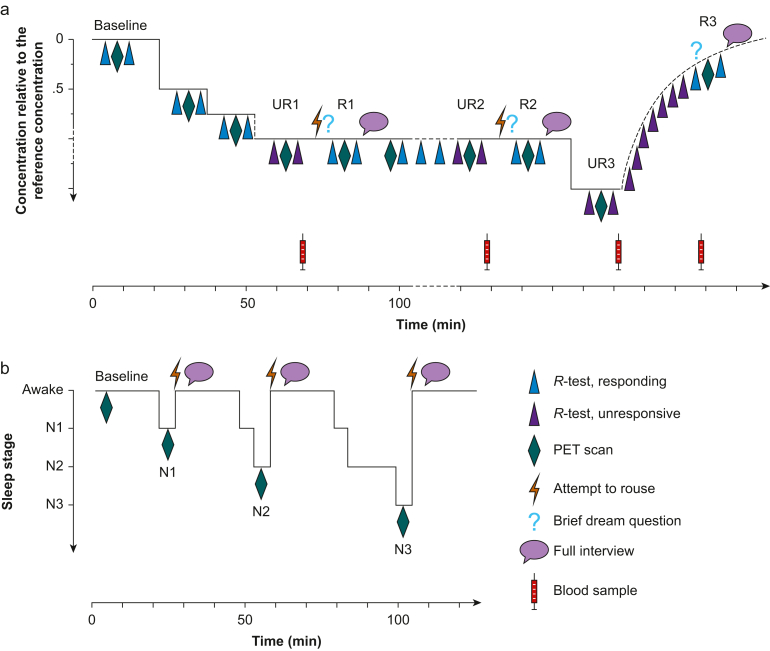
We compared, in a within-subject design, the prevalence and content of experiences in reports obtained after anaesthetic-induced unresponsiveness and NREM sleep. Healthy males (N=39) received dexmedetomidine (n=20) or propofol (n=19) in stepwise doses to induce unresponsiveness. Those rousable were interviewed and left unstimulated, and the procedure was repeated. Finally, the anaesthetic dose was increased 50%, and the participants were interviewed after recovery. The same participants (N=37) were also later interviewed after NREM sleep awakenings.
Most subjects were rousable, with no difference between anaesthetic agents (P=0.480). Lower drug plasma concentrations were associated with being rousable for both dexmedetomidine (P=0.007) and propofol (P=0.002) but not with recall of experiences in either drug group (dexmedetomidine: P=0.543; propofol: P=0.460). Of the 76 and 73 interviews performed after anaesthetic-induced unresponsiveness and NREM sleep, 69.7% and 64.4% included experiences, respectively. Recall did not differ between anaesthetic-induced unresponsiveness and NREM sleep (P=0.581), or between dexmedetomidine and propofol in any of the three awakening rounds (P>0.05). Disconnected dream-like experiences (62.3% vs 51.1%; P=0.418) and memory incorporation of the research setting (88.7% vs 78.7%; P=0.204) were equally often present in anaesthesia and sleep interviews, respectively, whereas awareness, signifying connected consciousness, was rarely reported in either state.
Anaesthetic-induced unresponsiveness and NREM sleep are characterised by disconnected conscious experiences with corresponding recall frequencies and content.
Clinical trial registration. This study was part of a larger study registered at ClinicalTrials.gov (NCT01889004).
麻醉诱导的无反应状态和非快速眼动(NREM)睡眠共享共同的神经通路和神经生理特征。我们假设这些状态在体验层面上也有相似之处。
我们在一项个体内设计中,比较了麻醉诱导无反应状态和 NREM 睡眠后报告中出现的体验的普遍性和内容。健康男性(N=39)接受右美托咪定(n=20)或丙泊酚(n=19)逐步剂量诱导无反应状态。可唤醒的患者接受采访并保持不被刺激,然后重复该过程。最后,将麻醉剂剂量增加 50%,并在恢复后对参与者进行采访。相同的参与者(N=37)之后也在 NREM 睡眠唤醒后接受了采访。
大多数受试者可被唤醒,两种麻醉剂之间无差异(P=0.480)。较低的药物血浆浓度与可唤醒的能力有关,无论是使用右美托咪定(P=0.007)还是丙泊酚(P=0.002),但与两种药物组的体验回忆无关(右美托咪定:P=0.543;丙泊酚:P=0.460)。在麻醉诱导无反应状态和 NREM 睡眠后进行的 76 次和 73 次采访中,分别有 69.7%和 64.4%包括体验。在麻醉诱导无反应状态和 NREM 睡眠之间,或在任何三个唤醒轮次中,右美托咪定和丙泊酚之间的回忆均无差异(P=0.581)。与 NREM 睡眠相比,麻醉诱导无反应状态下更常出现分离的梦境样体验(62.3%对 51.1%;P=0.418)和研究环境的记忆融合(88.7%对 78.7%;P=0.204),而在任何状态下都很少报告意识,表明存在连贯的意识。
麻醉诱导的无反应状态和 NREM 睡眠的特征是有意识的体验与相应的回忆频率和内容分离。
本研究是在 ClinicalTrials.gov(NCT01889004)注册的更大研究的一部分。