Aboye Genet Tadese, Vande Walle Martijn, Simegn Gizeaddis Lamesgin, Aerts Jean-Marie
M3-BIORES (Measure, Model & Manage Bioreponses), Division of Animal and Human Health Engineering, Department of Biosystems, KU Leuven, Leuven, Belgium.
School of Biomedical Engineering, Jimma University, Jimma, Oromia, Ethiopia.
Digit Health. 2023 May 29;9:20552076231178420. doi: 10.1177/20552076231178420. eCollection 2023 Jan-Dec.
The advent of digital systems and global mobile phone availability presents an opportunity for better healthcare access and equity. However, the disparity in the usage and availability of mHealth systems between Europe and Sub-Saharan Africa (SSA) has not been explored in relation to current health, healthcare status, and demographics.
This study aimed to compare mHealth system availability and use in SSA and Europe in the above-mentioned context.
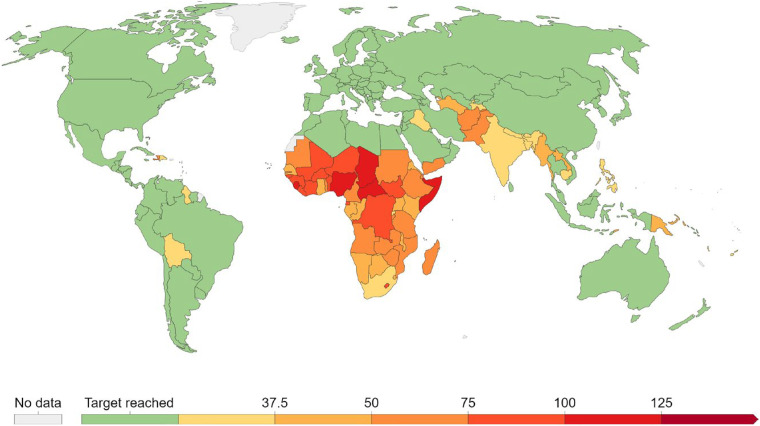
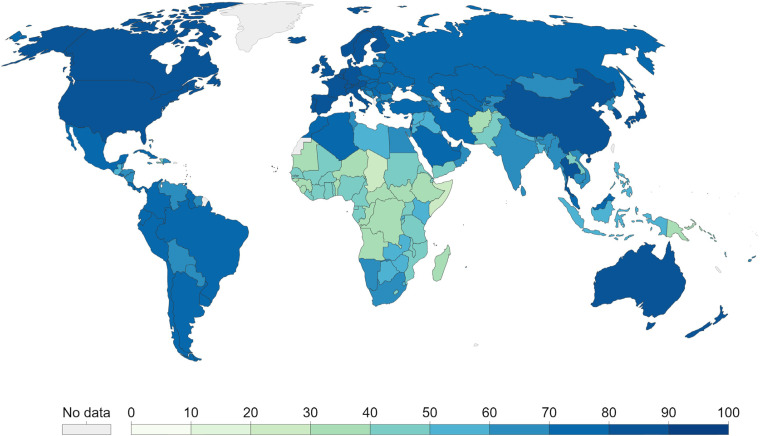
The study analyzed health, healthcare status, and demographics in both regions. It assessed mortality, disease burden, and universal health coverage. A systematic narrative review was conducted to thoroughly assess available data on mHealth availability and use, guiding future research in the field.
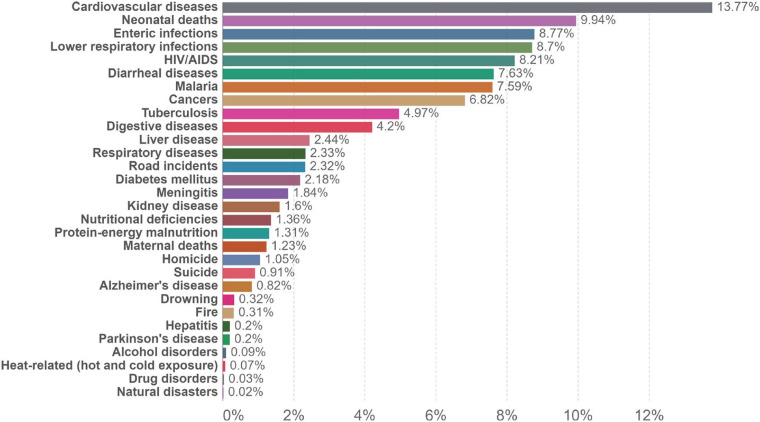
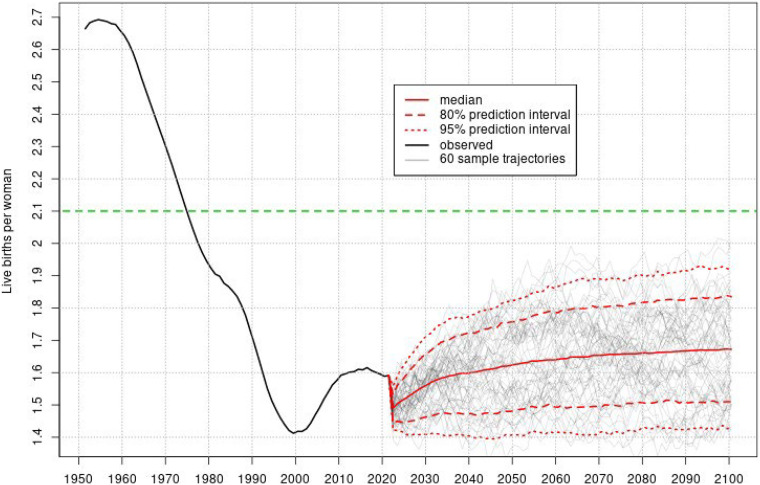
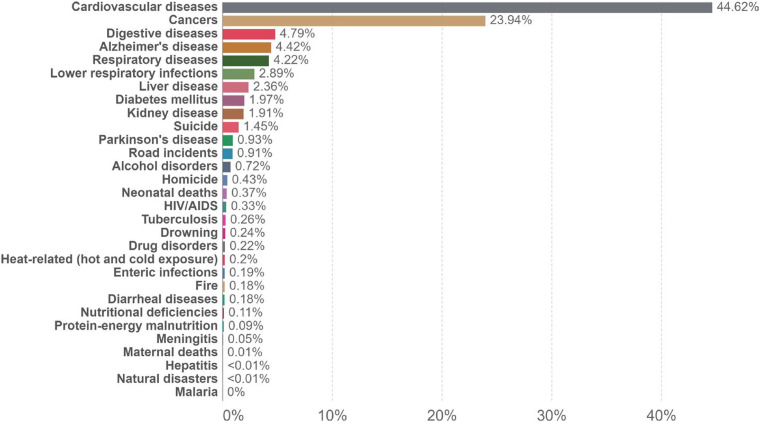
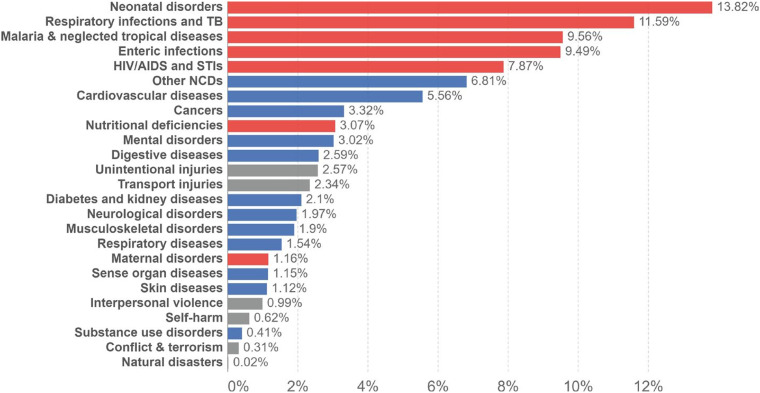
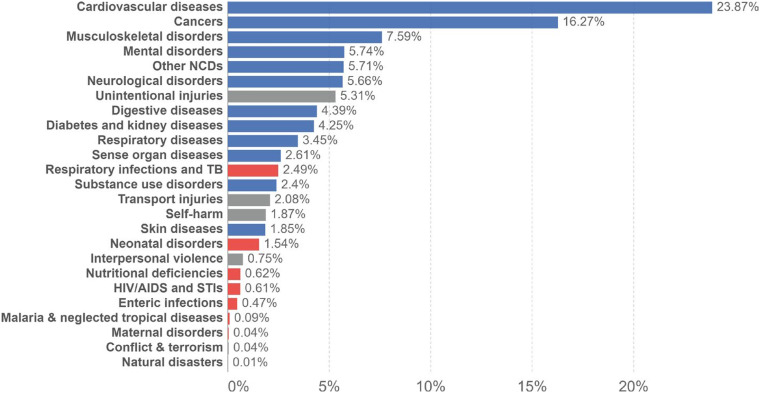
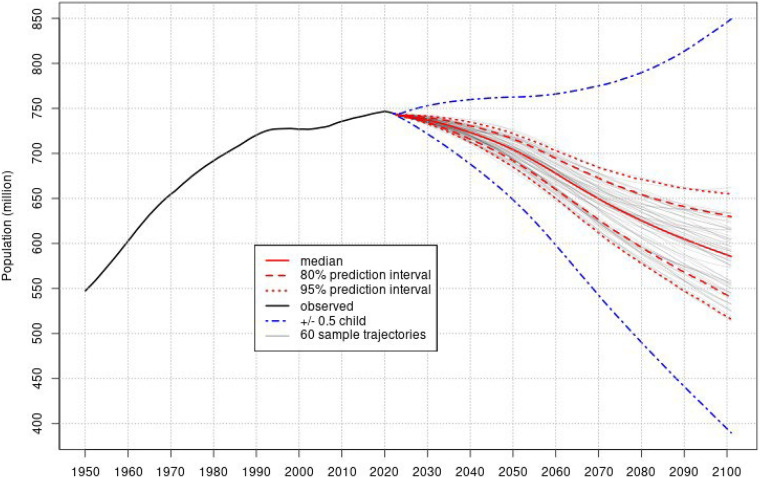
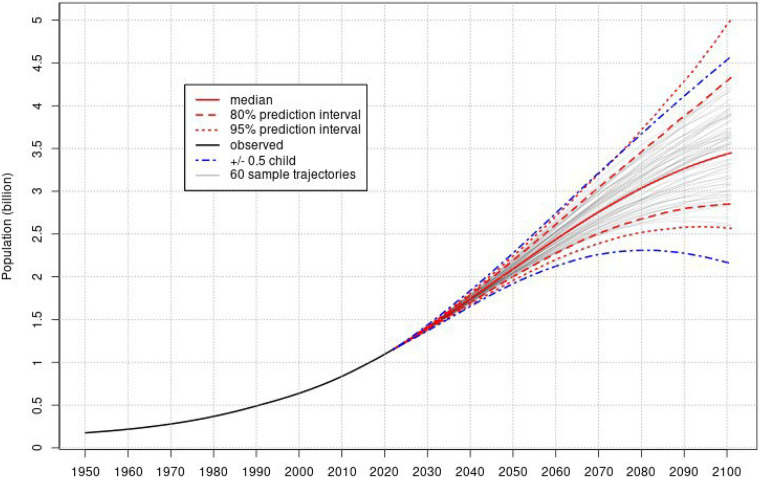
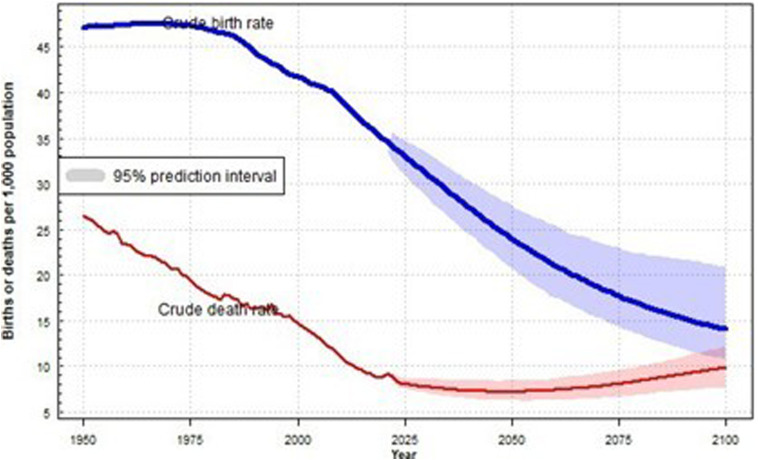
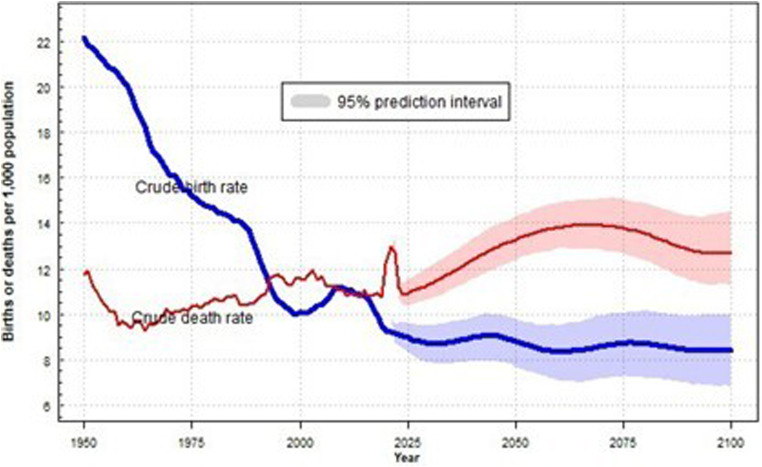
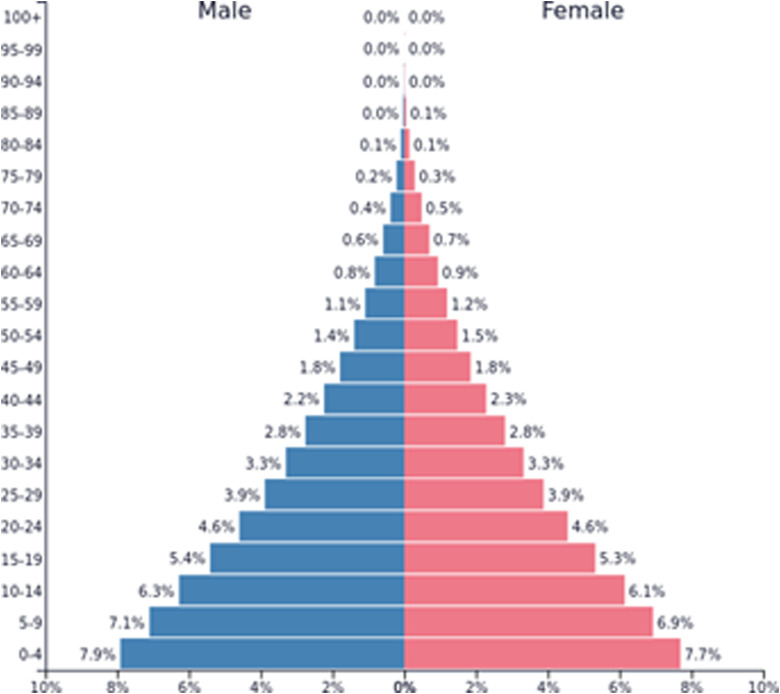
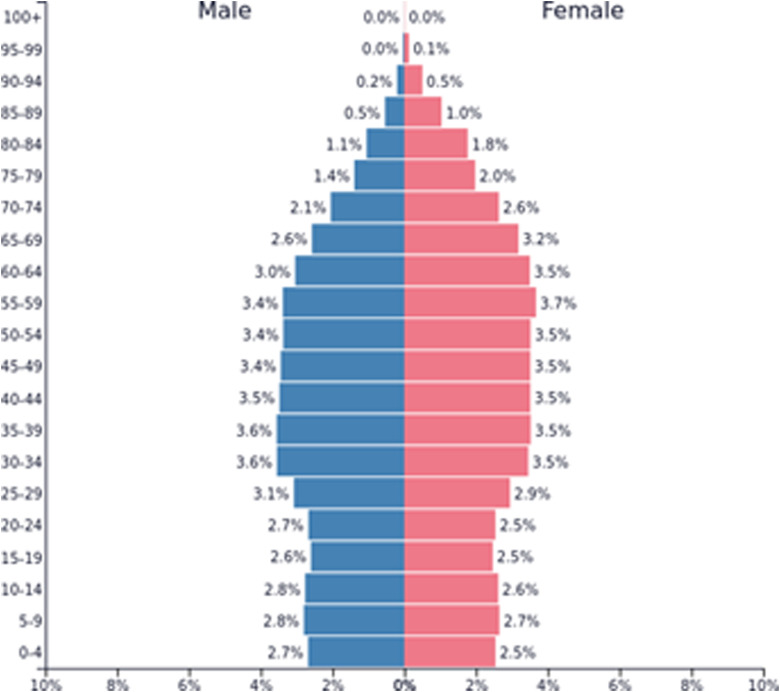
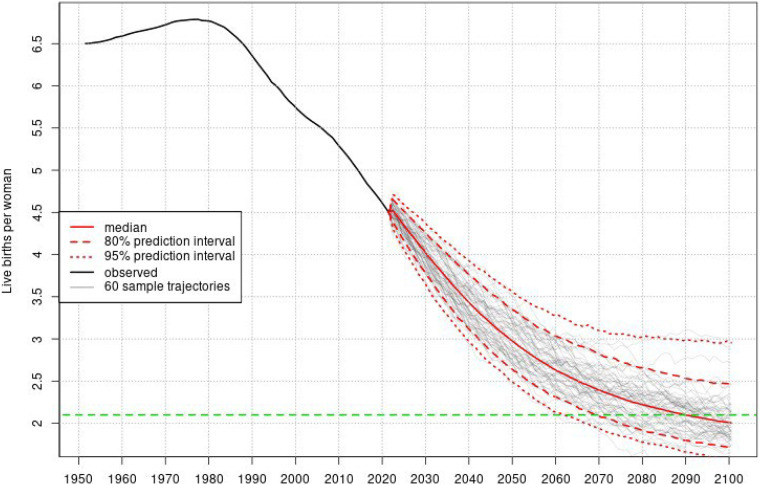
SSA is on the verge of stages 2 and 3 in the demographic transition with a youthful population and high birth rate. Communicable, maternal, neonatal, and nutritional diseases contribute to high mortality and disease burden, including child mortality. Europe is on the verge of stages 4 and 5 in the demographic transition with low birth and death rates. Europe's population is old, and non-communicable diseases (NCDs) pose major health challenges. The mHealth literature adequately covers cardiovascular disease/heart failure, and cancer. However, it lacks approaches for respiratory/enteric infections, malaria, and NCDs.
mHealth systems in SSA are underutilized than in Europe, despite alignment with the region's demographics and major health issues. Most initiatives in SSA lack implementation depth, with only pilot tests or small-scale implementations. Europe's reported cases highlight actual implementation and acceptability, indicating a strong implementation depth of mHealth systems.
数字系统的出现和全球手机的普及为改善医疗保健的可及性和公平性提供了契机。然而,欧洲与撒哈拉以南非洲(SSA)在移动健康(mHealth)系统的使用和可及性方面的差异,尚未结合当前的健康状况、医疗保健状况和人口统计学进行探讨。
本研究旨在比较上述背景下SSA和欧洲mHealth系统的可及性和使用情况。
该研究分析了两个地区的健康状况、医疗保健状况和人口统计学。评估了死亡率、疾病负担和全民健康覆盖情况。进行了系统的叙述性综述,以全面评估有关mHealth可及性和使用情况的现有数据,为该领域的未来研究提供指导。
SSA正处于人口转变的第2和第3阶段边缘,人口年轻化且出生率高。传染病、孕产妇、新生儿和营养疾病导致了高死亡率和疾病负担,包括儿童死亡率。欧洲正处于人口转变的第4和第5阶段边缘,出生率和死亡率较低。欧洲人口老龄化,非传染性疾病(NCDs)构成重大健康挑战。mHealth文献充分涵盖了心血管疾病/心力衰竭和癌症。然而,它缺乏针对呼吸道/肠道感染、疟疾和非传染性疾病的方法。
尽管SSA的mHealth系统与该地区的人口统计学和主要健康问题相契合,但与欧洲相比,其利用不足。SSA的大多数举措缺乏实施深度,只有试点测试或小规模实施。欧洲报告的案例突出了实际实施情况和可接受性,表明mHealth系统有很强的实施深度。