Ranjan Tulika, Yu Alexander, Elhamdani Shaed, Howard Candace M, Lirette Seth T, Denning Krista L, Valluri Jagan, Claudio Pier Paolo
Department of Neuro-oncology, Allegheny Health Network, Pittsburgh, Pennsylvania, USA.
Department of Neuro-Oncology, Cancer Center Southern Florida, and Tampa General Hospital, Tampa, Florida, USA.
Neurooncol Adv. 2023 May 12;5(1):vdad055. doi: 10.1093/noajnl/vdad055. eCollection 2023 Jan-Dec.
Glioblastoma (GBM) is a lethal disease. At least in part, the recurrence of GBM is caused by cancer stem cells (CSCs), which are resistant to chemotherapy. Personalized anticancer therapy against CSCs can improve treatment outcomes. We present a prospective cohort study of 40 real-world unmethylated Methyl-guanine-methyl-transferase-promoter GBM patients treated utilizing a CSC chemotherapeutics assay-guided report (ChemoID).
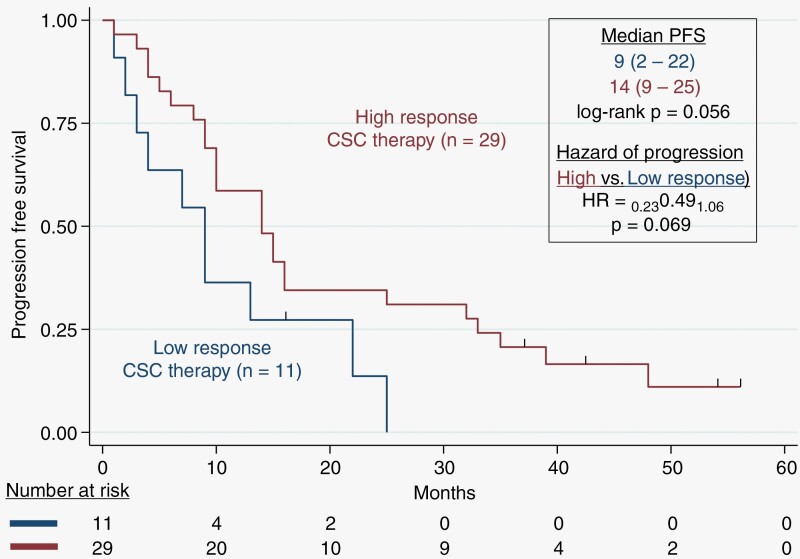
Eligible patients who underwent surgical resection for recurrent GBM were included in the study. Most effective chemotherapy treatments were chosen based on the ChemoID assay report from a panel of FDA-approved chemotherapies. A retrospective chart review was conducted to determine OS, progression-free survival, and the cost of healthcare costs. The median age of our patient cohort was 53 years (24-76).
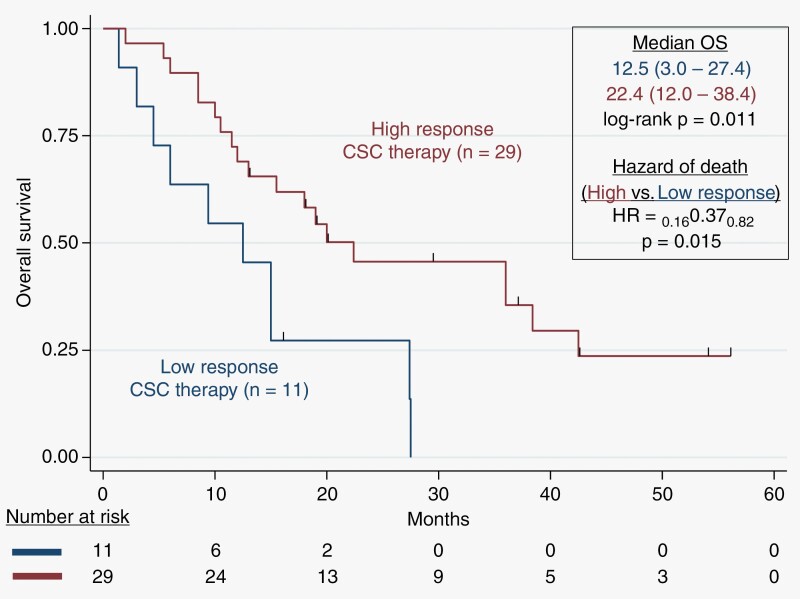
Patients treated prospectively with high-response ChemoID-directed therapy, had a median overall survival (OS) of 22.4 months (12.0-38.4) with a log-rank = .011, compared to patients who could be treated with low-response drugs who had instead an OS of 12.5 months (3.0-27.4 months). Patients with recurrent poor-prognosis GBM treated with high-response therapy had a 63% probability to survive at 12 months, compared to 27% of patients who were treated with low-response CSC drugs. We also found that patients treated with high-response drugs on average had an incremental cost-effectiveness ratio (ICER) of $48,893 per life-year saved compared to $53,109 of patients who were treated with low-response CSC drugs.
The results presented here suggest that the ChemoID Assay can be used to individualize chemotherapy choices to improve poor-prognosis recurrent GBM patient survival and to decrease the healthcare cost that impacts these patients.
胶质母细胞瘤(GBM)是一种致命疾病。GBM的复发至少部分是由对化疗耐药的癌症干细胞(CSC)引起的。针对CSC的个性化抗癌治疗可以改善治疗效果。我们开展了一项前瞻性队列研究,纳入了40例现实世界中甲基鸟嘌呤甲基转移酶启动子未甲基化的GBM患者,采用癌症干细胞化疗检测引导报告(ChemoID)进行治疗。
研究纳入了因复发性GBM接受手术切除的符合条件的患者。根据一组FDA批准的化疗药物的ChemoID检测报告选择最有效的化疗治疗方案。进行回顾性病历审查以确定总生存期(OS)、无进展生存期和医疗费用。我们患者队列的中位年龄为53岁(24 - 76岁)。
接受高反应性ChemoID导向治疗的患者,中位总生存期(OS)为22.4个月(12.0 - 38.4个月),对数秩检验P = 0.011,而接受低反应性药物治疗的患者OS为12.5个月(3.0 - 27.4个月)。接受高反应性治疗的复发性预后不良GBM患者12个月生存率为63%,而接受低反应性CSC药物治疗的患者为27%。我们还发现,与接受低反应性CSC药物治疗的患者相比,接受高反应性药物治疗的患者平均每挽救一个生命年的增量成本效益比(ICER)为48,893美元,而接受低反应性CSC药物治疗的患者为53,109美元。
此处呈现的结果表明,ChemoID检测可用于个体化化疗选择,以改善预后不良的复发性GBM患者的生存率,并降低影响这些患者的医疗费用。