Allama Iqbal Medical College, Lahore, Pakistan.
Marshfield Clinic Health System, Marshfield, WI, USA.
J Investig Med High Impact Case Rep. 2023 Jan-Dec;11:23247096231179448. doi: 10.1177/23247096231179448.
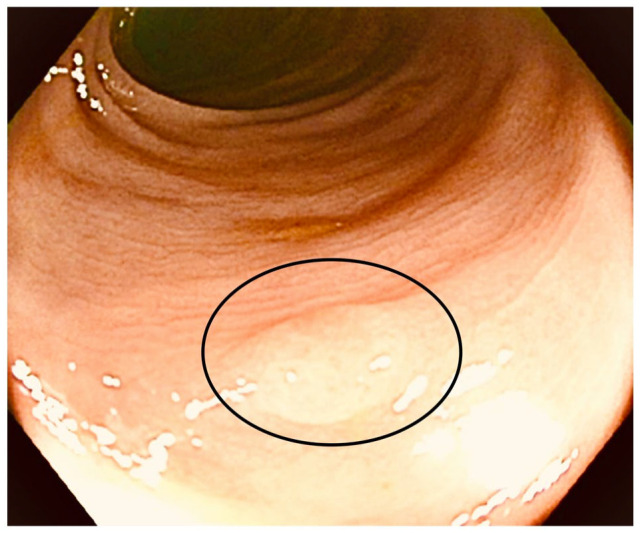
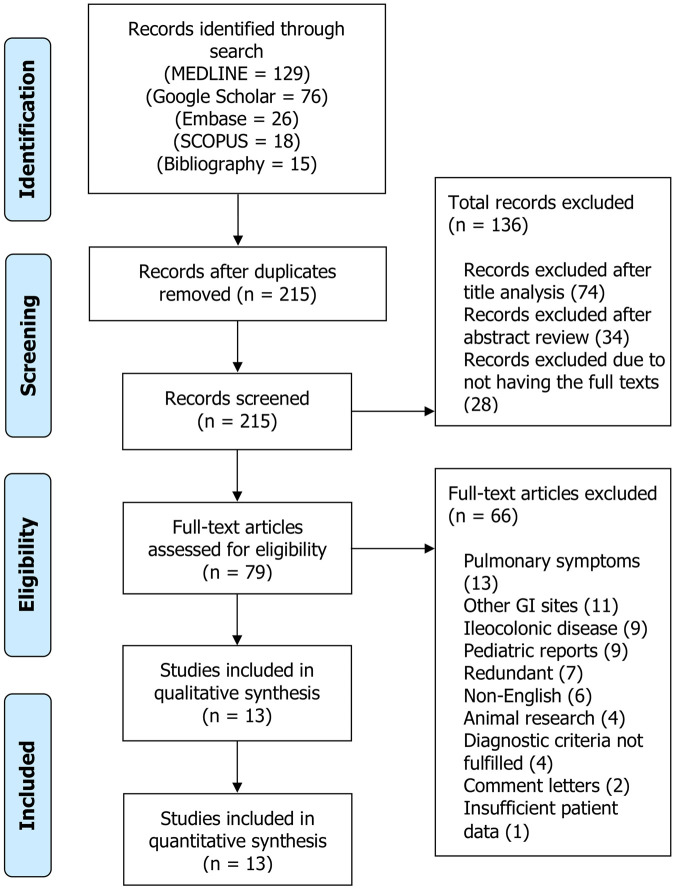
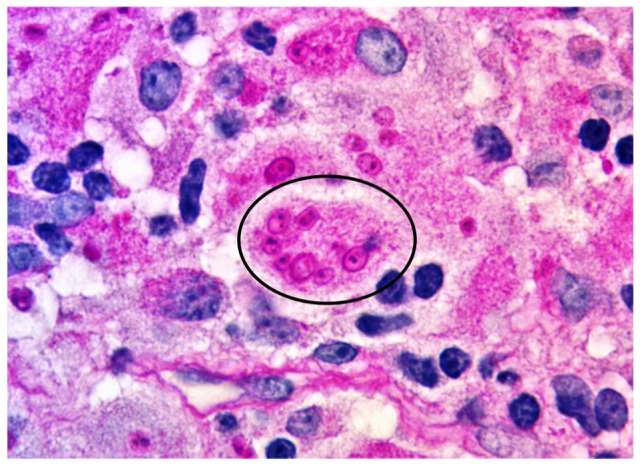
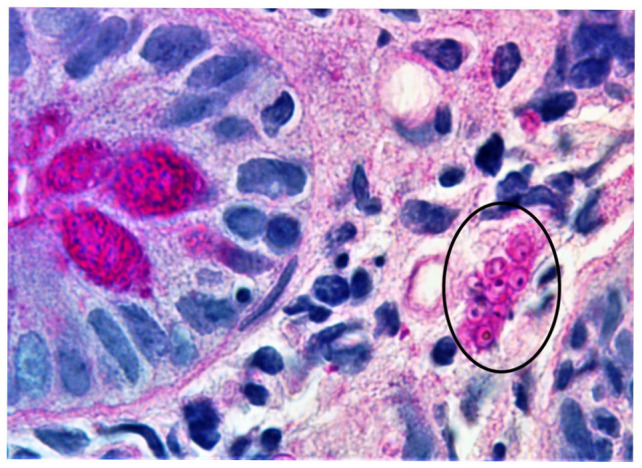
Gastrointestinal histoplasmosis remains an inconspicuous clinicopathologic entity. It is predominantly considered a protean manifestation of disseminated disease. We hereby delineate a unique case of biopsy-proven isolated colonic histoplasmosis in a patient undergoing methotrexate therapy. Furthermore, we present the first systematic review of the MEDLINE, Google Scholar, Embase, and Scopus databases regarding isolated colonic histoplasmosis in adult patients receiving immunomodulator therapy (IMT). A total of 13 case reports (level of clinical evidence: IV) were identified. The mean age was 55.6 ± 11.1 years, with 9 (69.2%) cases reported in women. Patients with subclinical disease (5, 38.5%) were often incidentally diagnosed by screening colonoscopy. Symptomatic individuals predominantly presented with diarrhea (4, 30.8%), weight loss (3, 23.1%), and/or abdominal pain (3, 23.1%). IMT was mainly administered for liver transplant (4, 30.8%), renal transplant (4, 30.8%), and ulcerative colitis (2, 15.4%). Common colonoscopy features included colonic ulcerations (7, 53.8%), polyps or pseudopolyps (3, 23.1%), and/or mass-like lesions (3, 23.1%). Diagnosis was made by histology of colonic biopsy in 11 (84.6%) and resected specimens in 2 (15.4%) patients. Treatment consisted of a combination of amphotericin B with oral itraconazole in 6 (46.2%), oral itraconazole alone in 5 (38.5%), and amphotericin B alone in 2 (15.4%) patients. Complete clinical recovery was achieved in all patients. This article illustrates that isolated colonic involvement can be the only clinical presentation of histoplasmosis. It may masquerade as other bowel disorders, presenting diagnostic and therapeutic conundrums. Gastroenterologists should rule out colonic histoplasmosis in IMT recipients who develop unexplained colitis symptoms.
胃肠道组织胞浆菌病仍然是一种不明显的临床病理实体。它主要被认为是播散性疾病的多种表现。在此,我们描述了一名接受甲氨蝶呤治疗的患者经活检证实的孤立性结肠组织胞浆菌病的独特病例。此外,我们对 MEDLINE、Google Scholar、Embase 和 Scopus 数据库进行了系统回顾,以了解接受免疫调节剂治疗(IMT)的成年患者中孤立性结肠组织胞浆菌病的情况。共确定了 13 例病例报告(临床证据水平:IV)。平均年龄为 55.6±11.1 岁,9 例(69.2%)报告为女性。无症状(5 例,38.5%)患者通常通过筛查性结肠镜检查偶然诊断。有症状的患者主要表现为腹泻(4 例,30.8%)、体重减轻(3 例,23.1%)和/或腹痛(3 例,23.1%)。IMT 主要用于肝移植(4 例,30.8%)、肾移植(4 例,30.8%)和溃疡性结肠炎(2 例,15.4%)。常见的结肠镜检查特征包括结肠溃疡(7 例,53.8%)、息肉或假性息肉(3 例,23.1%)和/或肿块样病变(3 例,23.1%)。11 例(84.6%)患者通过结肠活检和 2 例(15.4%)患者通过切除标本做出诊断。治疗方案包括两性霉素 B 联合口服伊曲康唑 6 例(46.2%)、单独口服伊曲康唑 5 例(38.5%)和单独两性霉素 B 2 例(15.4%)。所有患者均获得完全临床康复。本文表明,孤立性结肠受累可能是组织胞浆菌病的唯一临床表现。它可能伪装成其他肠道疾病,带来诊断和治疗上的难题。胃肠病学家应在接受 IMT 治疗后出现不明原因结肠炎症状的患者中排除结肠组织胞浆菌病。