PHMR Limited, London, UK.
Department of Applied Health Research, University College London, London, UK.
Pharmacoeconomics. 2023 Aug;41(8):1011-1025. doi: 10.1007/s40273-023-01281-8. Epub 2023 Jun 9.
Distributional cost-effectiveness analysis (DCEA) facilitates quantitative assessments of how health effects and costs are distributed among population subgroups, and of potential trade-offs between health maximisation and equity. Implementation of DCEA is currently explored by the National Institute for Health and Care Excellence (NICE) in England. Recent research conducted an aggregate DCEA on a selection of NICE appraisals; however, significant questions remain regarding the impact of the characteristics of the patient population (size, distribution by the equity measure of interest) and methodologic choices on DCEA outcomes. Cancer is the indication most appraised by NICE, and the relationship between lung cancer incidence and socioeconomic status is well established. We aimed to conduct an aggregate DCEA of two non-small cell lung cancer (NSCLC) treatments recommended by NICE, and identify key drivers of the analysis.
Subgroups were defined according to socioeconomic deprivation. Data on health benefits, costs, and target populations were extracted from two NICE appraisals (atezolizumab versus docetaxel [second-line treatment following chemotherapy to represent a broad NSCLC population] and alectinib versus crizotinib [targeted first-line treatment to represent a rarer mutation-positive NSCLC population]). Data on disease incidence were derived from national statistics. Distributions of population health and health opportunity costs were taken from the literature. A societal welfare analysis was conducted to assess potential trade-offs between health maximisation and equity. Sensitivity analyses were conducted, varying a range of parameters.
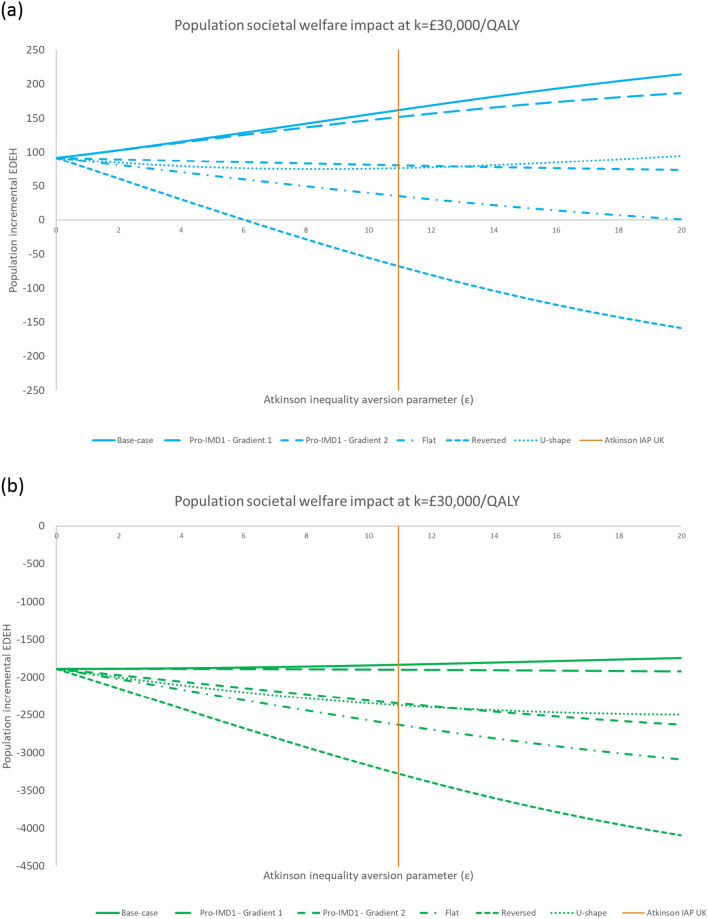
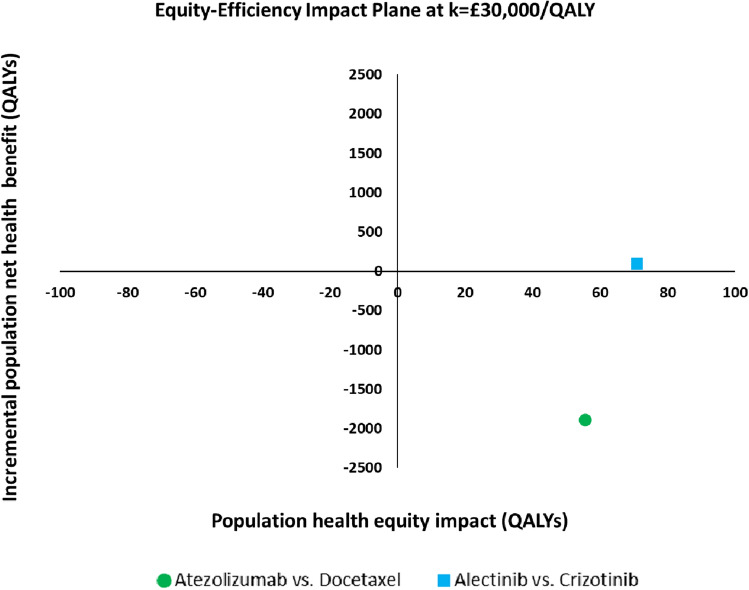
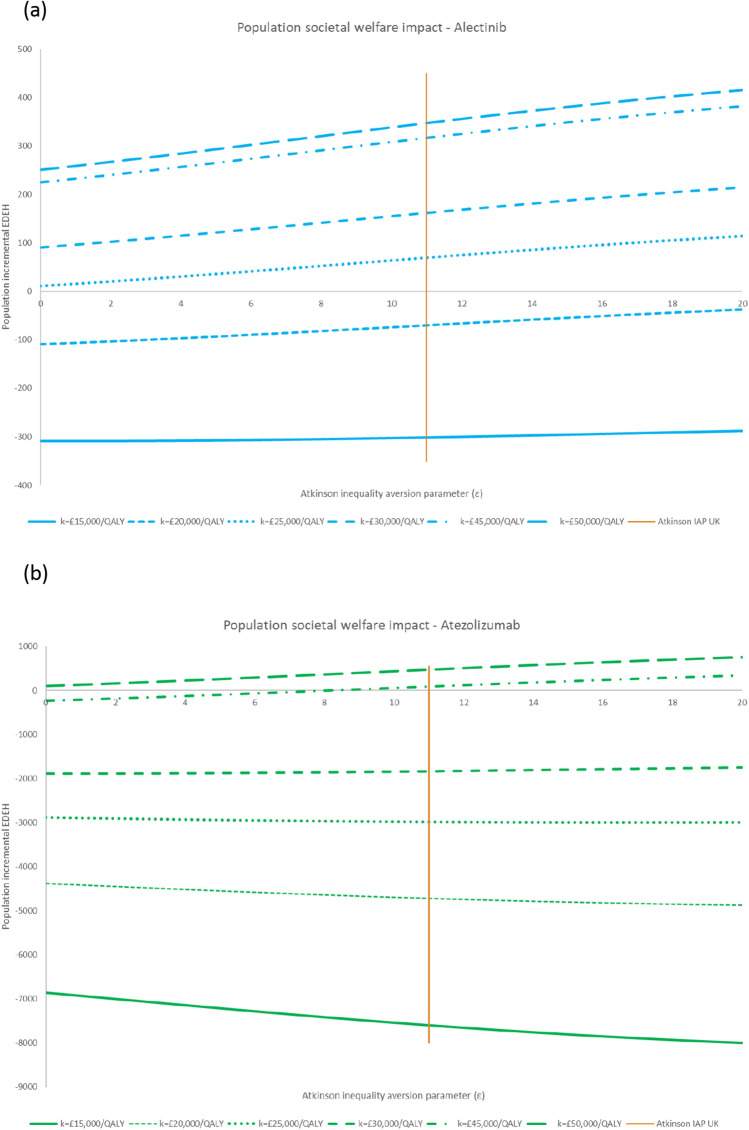
At an opportunity cost threshold of £30,000 per quality-adjusted life-year (QALY), alectinib improved both health and equity, thereby increasing societal welfare. Second-line atezolizumab involved a trade-off between improving health equity and maximising health; it improved societal welfare at an opportunity cost threshold of £50,000/QALY. Increasing the value of the opportunity cost threshold improved the equity impact. The equity impact and societal welfare impact were small, driven by the size of the patient population and per-patient net health benefit. Other key drivers were the inequality aversion parameters and the distribution of patients by socioeconomic group; skewing the distribution to the most (least) deprived quintile improved (reduced) equity gains.
Using two illustrative examples and varying model parameters to simulate alternative decision problems, this study suggests that key drivers of an aggregate DCEA are the opportunity cost threshold, the characteristics of the patient population, and the level of inequality aversion. These drivers raise important questions in terms of the implications for decision making. Further research is warranted to examine the value of the opportunity cost threshold, capture the public's views on unfair differences in health, and estimate robust distributional weights incorporating the public's preferences. Finally, guidance from health technology assessment organisations, such as NICE, is needed regarding methods for DCEA construction and how they would interpret and incorporate those results in their decision making.

分布成本效益分析(DCEA)有助于定量评估健康效果和成本在人群亚组中的分布情况,以及在最大化健康和公平之间的潜在权衡。英国国家卫生与保健优化研究所(NICE)目前正在探索 DCEA 的实施。最近的研究对 NICE 评估中的一系列选择进行了综合 DCEA;然而,对于患者人群特征(大小、按感兴趣的公平衡量标准分布)和方法选择对 DCEA 结果的影响,仍存在重大问题。癌症是 NICE 评估最多的指征,肺癌发病率与社会经济地位之间的关系已得到充分确立。我们旨在对 NICE 推荐的两种非小细胞肺癌(NSCLC)治疗方法进行综合 DCEA,并确定分析的关键驱动因素。
根据社会经济剥夺程度对亚组进行定义。从两项 NICE 评估中提取健康效益、成本和目标人群数据(阿特珠单抗与多西他赛[化疗后二线治疗代表广泛的 NSCLC 人群]和阿来替尼与克唑替尼[靶向一线治疗代表罕见的突变阳性 NSCLC 人群])。疾病发病率数据来自国家统计数据。人群健康和健康机会成本的分布情况取自文献。进行社会福利分析,以评估在最大化健康和公平之间的潜在权衡。进行了敏感性分析,改变了一系列参数。
在机会成本阈值为每质量调整生命年(QALY)30,000 英镑的情况下,阿来替尼提高了健康和公平性,从而提高了社会福利。二线阿特珠单抗在改善健康公平和最大化健康之间存在权衡;在机会成本阈值为每 QALY50,000 英镑时,它提高了社会福利。提高机会成本阈值改善了公平性影响。公平性影响和社会福利影响很小,这是由患者人群的大小和每位患者的净健康效益驱动的。其他关键驱动因素是不平等厌恶参数和按社会经济群体划分的患者分布情况;将分布向最(最)贫困五分位数倾斜,可提高(降低)公平收益。
使用两个说明性示例并改变模型参数来模拟替代决策问题,本研究表明,综合 DCEA 的关键驱动因素是机会成本阈值、患者人群特征和不平等厌恶程度。这些驱动因素提出了重要的问题,涉及对决策的影响。需要进一步研究来检验机会成本阈值的价值,捕捉公众对健康不公平差异的看法,并估计包含公众偏好的稳健分布权重。最后,需要卫生技术评估组织(如 NICE)提供有关 DCEA 构建方法的指导,以及他们将如何解释和将这些结果纳入其决策。