Zeng Haiyan, Tohidinezhad Fariba, De Ruysscher Dirk K M, Willems Yves C P, Degens Juliette H R J, van Kampen-van den Boogaart Vivian E M, Pitz Cordula, Cortiula Francesco, Brandts Lloyd, Hendriks Lizza E L, Traverso Alberto
Department of Radiation Oncology (Maastro), GROW School for Oncology and Reproduction, Maastricht University Medical Centre+, 6229 ET Maastricht, The Netherlands.
Department of Respiratory Medicine, Zuyderland Medical Center, 6419 PC Heerlen, The Netherlands.
Cancers (Basel). 2023 May 31;15(11):3010. doi: 10.3390/cancers15113010.
To identify clinical risk factors, including gross tumor volume (GTV) and radiomics features, for developing brain metastases (BM) in patients with radically treated stage III non-small cell lung cancer (NSCLC).
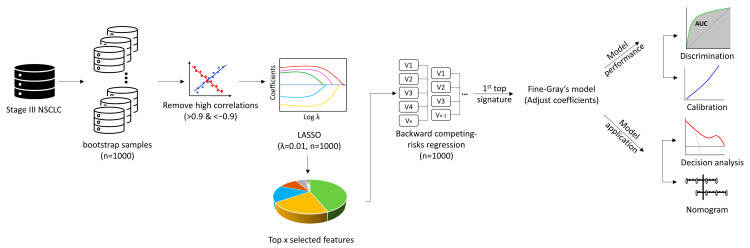
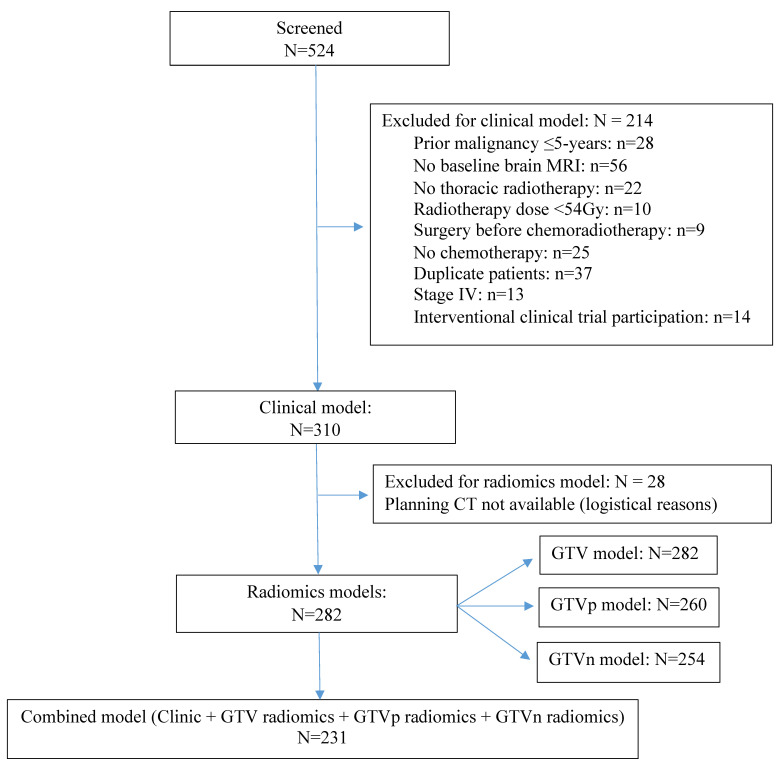
Clinical data and planning CT scans for thoracic radiotherapy were retrieved from patients with radically treated stage III NSCLC. Radiomics features were extracted from the GTV, primary lung tumor (GTVp), and involved lymph nodes (GTVn), separately. Competing risk analysis was used to develop models (clinical, radiomics, and combined model). LASSO regression was performed to select radiomics features and train models. Area under the receiver operating characteristic curves (AUC-ROC) and calibration were performed to assess the models' performance.
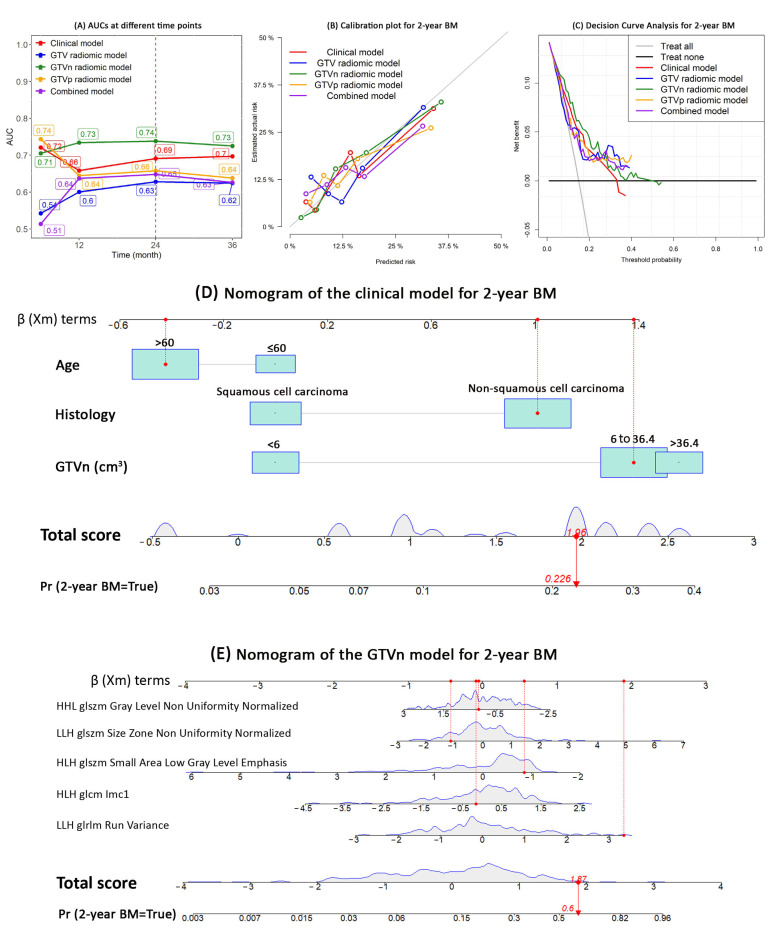
Three-hundred-ten patients were eligible and 52 (16.8%) developed BM. Three clinical variables (age, NSCLC subtype, and GTVn) and five radiomics features from each radiomics model were significantly associated with BM. Radiomic features measuring tumor heterogeneity were the most relevant. The AUCs and calibration curves of the models showed that the GTVn radiomics model had the best performance (AUC: 0.74; 95% CI: 0.71-0.86; sensitivity: 84%; specificity: 61%; positive predictive value [PPV]: 29%; negative predictive value [NPV]: 95%; accuracy: 65%).
Age, NSCLC subtype, and GTVn were significant risk factors for BM. GTVn radiomics features provided higher predictive value than GTVp and GTV for BM development. GTVp and GTVn should be separated in clinical and research practice.
识别接受根治性治疗的Ⅲ期非小细胞肺癌(NSCLC)患者发生脑转移(BM)的临床风险因素,包括肿瘤总体积(GTV)和影像组学特征。
从接受根治性治疗的Ⅲ期NSCLC患者中检索胸部放疗的临床资料和计划CT扫描图像。分别从GTV、原发性肺肿瘤(GTVp)和受累淋巴结(GTVn)中提取影像组学特征。采用竞争风险分析建立模型(临床模型、影像组学模型和联合模型)。进行LASSO回归以选择影像组学特征并训练模型。采用受试者操作特征曲线下面积(AUC-ROC)和校准来评估模型性能。
310例患者符合条件,52例(16.8%)发生BM。三个临床变量(年龄、NSCLC亚型和GTVn)以及每个影像组学模型的五个影像组学特征与BM显著相关。测量肿瘤异质性的影像组学特征最为相关。模型的AUC和校准曲线显示,GTVn影像组学模型性能最佳(AUC:0.74;95%CI:0.71-0.86;灵敏度:84%;特异度:61%;阳性预测值[PPV]:29%;阴性预测值[NPV]:95%;准确度:65%)。
年龄、NSCLC亚型和GTVn是BM的重要风险因素。GTVn影像组学特征对BM发生的预测价值高于GTVp和GTV。在临床和研究实践中应将GTVp和GTVn区分开来。